All published articles of this journal are available on ScienceDirect.

Association of Genital Chlamydia trachomatis Infection with Female Infer-tility, Study in a Tertiary Care Hospital in Eastern India
Authors Info & Affiliations
Abstract
Background : Chlamydia trachomatis is recognized as one of the most common sexually transmitted pathogen in the world. 50-80% of infected females are asymptomatic. These untreated women are at risk of developing chronic sequelae leading to tubal pathology causing infertility. Infertility is defined as 1 year of unprotected intercourse without pregnancy. It may be primary or secondary. Aim : To find out the association of genital Chlamydia trachomatis infection with female infertility. Materials and Methodology : This case control study has been carried out in collaboration with R. G. Kar Medical College and Institute of Post Graduate Medical Education & Research, India, between July 2012 and June 2013. 40 infertile and 40 pregnant women were enrolled by purposive sampling as per inclusion and exclusion criteria. ELISA test was performed to detect serum IgG and IgA antibody against recombinant analogs of MOMP and 3 different PCR assays were done targeting MOMP and rRNA DNA from DNA extracted from first void urine. Results : IgG seropositivity was significantly higher (15% vs 0%, P=.0255) in cases than controls, though there was no significant difference in the proportion of IgA seropositivity among 2 groups (12.5% vs 2.5%, P=0.2007). Out of 80 samples 2 samples showed the production of amplicons with R1 – R2 primers. Only 1 sample gave positive result with production of amplicons with all the 3 primers used (R1 – R2, CT0005 – CT06 and JM15 – JM16). Conclusion : Persistent C. trachomatis infection must be recognized as a risk factor of infertility in this region of India. The low PCR positivity in FVU sample helps to conclude the diagnostic utility of serological tests in screening of infertile women.
INTRODUCTION
Chlamydia trachomatis is an obligate intracellular bacterium. It is currently recognized as one of the most common sexually transmitted pathogen. World Health Organization (WHO) estimates that, globally 98 million adults were infected by C. trachomatis at any point of time in the year 2005 [1]. According to U.S. Centre for Disease Control (CDC) and Prevention STD surveillance report 2007, 1,030,911 Chlamydia trachomatis infection were reported in 2006, which increased to about 1.24 millions in the year 2009 [2, 3]. Due to lack of screening in some population and little public awareness there is substantial underreporting. CDC estimates that 2-3 million new cases occur every year [3].
Acute genital tract infections due to Chlamydia trachomatis serovars D through K are associated with many syndromes like cervicitis, salpingitis, acute urethral syndrome and endometritis in females or urethritis, proctitis and epididymitis in males [4]. These infections can be treated and controlled, if proper and timely medical intervention is made. These may lead to major complications like chronic pelvic pain, pelvic inflammatory disease (PID), ectopic pregnancy and tubal factor infertility. According to different studies 50 - 80% of female patients with genital Chlamydia trachomatis infection lack symptom [5]. Thus a large reservoir of infected people continue to transmit it sexually and also is at risk of different sequelae in any given population. It is primarily a woman’s health care issue since the manifestations and consequences are more damaging to the reproductive health in woman than in man.
Infertility is defined as 1 year of unprotected intercourse without pregnancy. It is further classified as primary and secondary infertility. Primary infertility is a term used to designate those couples who have never conceived, whereas secondary infertility is a term used for a condition where a prior pregnancy, although not necessarily a live birth has occurred [6]. Infertility has a great socio-psychological impact. According to a joint WHO-DHS comparative report in 2004, 60-80 million couples suffer from infertility worldwide [7]. Prevalence varies across different regions of the world and is estimated to affect 8% to 12% of couples worldwide [8]. Overall prevalence of primary infertility in India is between 3.9% and 16.8% [7].
The target cells of genital tract infections in women are squamo-columnar epithelial cells of the endocervix and upper genital tract [4]. Infection of reproductive tract epithelium results in production of interleukin (IL)-1, tumor necrosis factor-α (TNF-α), IL-8, growth-related oncogene (GRO)–a, granulocyte-macrophage colony stimulating factor (GM-CSF), and IL-6, which induce increased expression of endothelial adhesion molecules that aid in the attraction of immune cells [4, 9-11]. Resident tissue macrophages also contribute to early release of cytokines and chemokines. Infected epithelial cells release matrix metalloproteases (MMPs) which contribute to tissue proteolysis and remodeling. At the time of reinfection, host cells’ release of chemokines leads to recruitment of Chlamydia specific immune cells that rapidly amplify the response [12]. Chlamydial endometritis and salpingitis induces antibodies to heat shock proteins (hsps), particularly, hsp 60 [9, 13]. As Chlamydia shares epitopes with human hsps, it may cause an autoimmune response [4, 14, 15]. Reticulate bodies may escape the immune response, and causes persistent infection. Host, virulence of the pathogen and environment are the determining factors for the clearance or persistence of the infection [16]. Formation of new elementary bodies from reticulate bodies can induce immune response and inflammatory reactions resulting in a cyclic process of scarring of the infected tissue leading to partial or total obliteration of the fallopian tubes causing tubal factor infertility or sub infertility [12, 14, 17]. After one episode of Pelvic Inflammatory Disease (PID) the ratio of infertility has been estimated to be 25% which increases to 50% and 75% after 2nd and 3rd episodes respectively [14].
Chlamydial PID is one of the most common preventable causes of tubal factor infertility and adverse pregnancy outcomes. Exact scenario about prevalence of genital Chlamydia trachomatis infection and its sequelae is scarce in developing countries as reliable tests are too expensive and complex to carry out as routine screening methods.
The present study was conducted to find out the association of genital tract Chlamydia trachomatis infection with female infertility by evaluating the magnitude of infection in infertile and pregnant women.
MATERIALS AND METHODOLOGY
The present case control study has been carried out in collaboration with Department of Microbiology and Department of Gynaecology & Obstetrics (G & O), R. G. Kar medical college, Kolkata 700004, India and Biochemistry research wing, Department of Biochemistry, Institute of Post Graduate Medical Education & Research, Kolkata 700020, India, from July 2012 to June 2013.
Infertile women (cases n1 = 40) attending Gynaecology Out Patient Department (OPD) were enrolled by purposive sampling as per inclusion and exclusion criteria. Sample size was determined by the Fleiss method [18] with continuity correction from Open Epi, Version 3, open source calculator--SSCC considering the study of Malik et al., 2006 as reference [19]. Cases of primary and secondary female infertility with or without history of pelvic inflammatory disease (PID), associated laparoscopic findings like tubal blockage, adhesion etc. were included in the study. Diagnosed cases of female infertility due to other reasons such as endometriosis, polycystic ovarian disease, PID due to other causes, mechanical causes of infertility (previous surgery, dilatation & curettage, congenital abnormalities etc.), and medical disorders were excluded from the present study. Pregnant women (n2 = 40) attending Antenatal clinic were included in the study as controls. The cases and controls were matched according to their mean age and socio economic status (as per modified B.G. Prasad’s scale, 2013) [20]. Institutional ethics committee (IEC) clearance was obtained. Informed consent form duly signed by all the subjects was obtained after explanation of purpose of study.
Laboratory Investigations
Enzyme Linked Immuno Sorbent Assay (ELISA)
Serum samples were tested for the detection of IgG and IgA antibodies to C. trachomatis by using commercially available kits (DS-EIA-ANTI-CHLAMYDIA TR-A Kit/ DS-EIA-ANTI-CHLAMYDIA TR-G Kit, DSI, Germany). The antigens used in these assays are recombinant analog of major outer membrane protein (MOMP) of C. trachomatis. The test was validated according to the kit manual. The optical density was read at 450 nm using a microplate reader. Cut off value was calculated according to the manufacturer’s instructions.
Polymerase Chain Reaction
15 ml of first void urine was collected aseptically in a sterile falcon (USA) polypropelene centrifuge tube and stored immediately at 4°C. None of the patients had received antibiotic treatment 4 weeks prior to the visit and were eligible if they had not voided urine during the last 2 hours. The samples were centrifuged at 1400 g for 20 minutes. The supernatant was discarded and the pellet was dissolved in 1 x Phosphate Buffer Saline (PBS; pH 7.4) solution and stored at –200C until DNA extraction was done.
DNA was extracted according to the modified method described by Fallah et al., 2005 [21]. In brief, the stored urine sample was centrifuged at 8900 g for 5 minutes in a microcentrifuge tube at room temperature. The pellet was dissolved in 500µl of lysis buffer [pH 7.5, 50mM TrisEDTA (sigma, USA), 1% SDS (sigma, USA)] and incubated at 55°C in a dry bath for overnight. After overnight incubation the lysed cells in buffer was centrifuged at 8900 g for 10 minutes in a microcentrifuge. The pellet was dissolved in 200µl of Tris EDTA Glucose buffer [pH 7.0, 25mM Tris (sigma, USA), 10mM EDTA (Sigma, USA), 50mM glucose (Sigma, USA), 20 µl Proteinase K (20mg/ml, Sigma, USA) ] and 200µl of Absolute ethanol (Sigma, USA, 95 – 100%). Then it was mixed thoroughly by vortexing for 15 seconds and was incubated at 370C for 10 minutes. The lysate was transferred into a HiElute Miniprep Spin column (MB505 HiPura Bacterial and Yeast Genomic DNA Purification Spin Kit, Himedia, India) and centrifuged at 8900 g for 1 minute. Further DNA was extracted according to instructions of manufacturer (MB505 HiPura Bacterial and Yeast Genomic DNA Purification Spin Kit, HiMedia India). The eluted DNA was identified by electrophoresis on 1% agarose gel, stained with 0.5 mg/ml ethidium bromide, in 1X Tris-Acetate EDTA buffer (pH 8.0). The purity of extracted DNA was determined by measuring the quotient of the absorption data measured at 260nm and 280 nm by using a UV visible double beam spectrophotometer.
3 different PCR assays targeted a major outer membrane protein (MOMP) and rRNA DNA. For analysing MOMP and rRNA DNA, 100 ng DNA was amplified with the use of 1 unit DNA polymerase (Fermentus) in PCR reaction mixture, containing 1X PCR buffer (10mM Tris, pH 8.3, 50mM KCl, 2.5mM MgCl2, 0.01% gelatin), 2 mM MgCl2, 0.25 mM each dNTP, 20 picomoles each forward and reverse primers. The primer sequences, primer annealing temperature (Ta0) and PCR product sizes were given in Table 1. The PCR reaction was performed using following condition: 94oC, 5 minutes, followed by 30 cycles of 94oC for 1 minute, Ta0 for respective primers (Table 1) for 1 minute, 72oC for 1 minute and followed by 72oC for 10 minutes for final extension. The amplified products were separated by electrophoresis on 1.5% agarose gel, stained with 0.5 mg/ml ethidium bromide, in 1X Tris Acetate EDTA buffer (pH 8.0). The PCR products were visualized and photographed under UV transilluminator using a computer assisted image analysis program (UVP Doc. It ® LS Image Analysis Software; version 6.3.3).
RESULTS
Age
The analysis revealed that the overall mean age of the participants were 24.85 ± 4.51 years. The respective values among the cases and controls were found to be 24.88 ± 4.97 years Vs 24.83 ± 4.05 years with a statistically insignificant difference (P = .96).
Distribution of Infertile Patients According to Primary and Secondary Infertility
75% (n1 = 30) of cases were suffering from primary infertility and rest (n2 = 10; 25%) from secondary infertility.
Result of PCR
Test revealed relatively low and equal magnitude among pregnant (2.5%) and infertile (2.5%) women. Naturally there was no statistically significant difference between the two groups (P = 1.0). Out of 80 samples 2 samples (I15 and P6) showed the production of amplicons that had base pairs of molecular weight 208bp with R1 – R2 primers (Fig. 1). Only 1 sample (I15) gave positive result with production of amplicons of 208bp, 280bp & 208bp respectively with all the 3 primers used, i.e, R1 – R2 (Fig. 1), JM15 – JM16 (Fig. 2) & CT0005 – CT06 (Fig. 3).
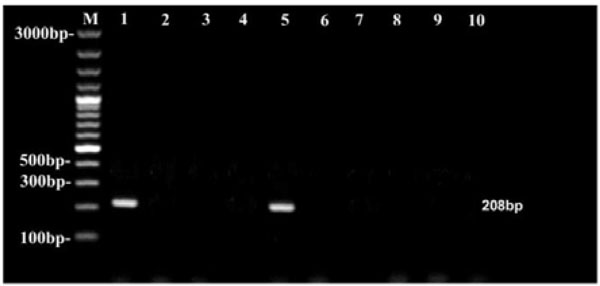
Agarose gel electrophoresis of amplified products with R1 – R2 primer. DNA marker is in the left outside lane. Lane 1 (I15) and Lane 5 (P6) show amplified product of 208bp.
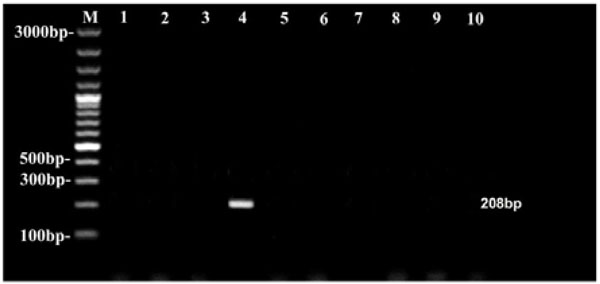
Agarose gel electrophoresis of amplified products with JM15 – JM16 primer. DNA marker is in the left outside lane. Lane 4 (I15) shows amplified product of 208bp.
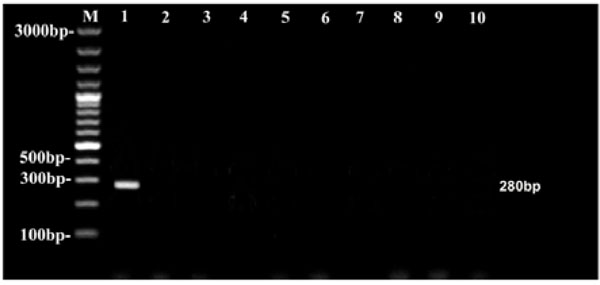
Agarose gel electrophoresis of amplified products with CT0005-CT06 primer. DNA marker is in the left outside lane. Lane 1 (I15) shows amplified product of 280bp.
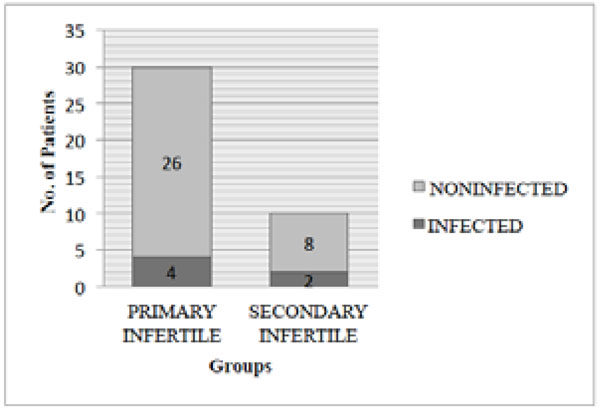
Component bar diagram showing magnitude of Chlamydia trachomatis infection among primary and secondary infertile cases.
Primer sequence and condition used for PCR method.
| Primer name | Primer sequence (5’ – 3’) | Product size (bp) | Ta0 |
|---|---|---|---|
| CT0005 – CT06 [22, 23] | CT0005 – 5’ GAT AGC CAG CAC AAA GAG AG 3’ CT06 – 5’ CTT TGT TTT CGA CCG TGT TTT 3’ |
280 | 550C |
| JM15 – JM16 [23] | JM15 – 5’ TTG CTT GGA GTG CTG GACT 3’ JM16 – 5’ TCC TTA GTT CCT GTC ACA CC 3’ |
208 | 550C |
| R1 – R2 [24, 25] | R1 – 5’ GTG GAT AGT CTC AAC CCT AT 3’ R2 – 5’ TAT CTG TCC TTG CGG AAA AC 3’ |
208 | 420C |
Distribution of infertile and pregnant women as per different socioeconomic status (as per modified B. G. Prasad’s scale, 2013) [20] (N = 80).
| Groups | Class I No. (%) |
Class II No. (%) |
Class III No. (%) |
Class IV No. (%) |
Class V No. (%) |
Total | x2, df, P |
|---|---|---|---|---|---|---|---|
| Infertile (n1 = 40) |
3 (7.5) | 18 (45.0) | 9 (22.5) | 10 (25.0) | 0 (0.0) | 40 (100.0) | 9.301, 4, 0.0540 |
| Pregnant (n2 = 40) |
0 (0.0) | 10 (25.0) | 11 (27.5) | 17 (42.5) | 2 (5.0) | 40 (100.0) | |
| Total (N = 80) |
3 (3.75) | 28 (35.0) | 20 (25.0) | 27 (33.75) | 2(2.5) | 80 (100.0) | -------------- |
* Chi square test performed. df: degree of freedom
Distribution of participants as per their IgG seropositivity status (N = 80).
| IgG | Infertile [n1=40] No (%) |
Pregnant [n2=40] No (%) |
Total [N=80] No (%) |
P [Fisher’s exact test], OR* (95%CI) |
|---|---|---|---|---|
| Present | 6 (15.0) | 0 (0.0) | 6 (7.5) | 0.02, 15.26 (0.8290 – 280.9) |
| Absent | 34 (85.0) | 40 (100.0) | 74 (92.5) | |
| Total | 40 (100.0) | 40 (100.0) | 80 (100.0) | ----------------------------- |
* OR: Odds Ratio, CI: Confidence Interval
* The above table shows that despite the significantly (as per Fisher exact test) higher rate of IgG seropositivity in the infertile group the difference was not shown to be statistically robust as per 95% CI of OR. However, it was revealed to be significant at 90% confidence interval (90% CI 1.324 to 175.8).
Distribution of participants as per their IgA seropositivity status (N = 80).
| IgA | Infertile [n1=40] No (%) |
Pregnant [n2=40] No (%) |
Total [N=80] No (%) |
P [Fisher’s exact test], OR* (95%CI) |
|---|---|---|---|---|
| Present | 5 (12.5) | 1 (2.5) | 6 (7.5) | 0.2, 5.571 (0.6201 – 50.06) |
| Absent | 35 (87.5) | 39 (97.5) | 74 (92.5) | |
| Total | 40 (100.0) | 40 (100.0) | 80 (100.0) | ----------------------------- |
* OR: Odds Ratio, CI: Confidence Interval
Based on results of serological tests and PCR total 7 (8.75%) patients were diagnosed as infected. Among the 6 infected infertile patients, 4 were suffering from primary infertility and 2 from secondary infertility (Diagram 1).
There was no statistically significant difference in the infectivity rate between primary infertile (13.33%) and secondary infertile (20.00%) patients (Fisher’s exact test, p = 0.6287, OR = 0.6154 95% CI 0.09449 to 4.008). The only infected pregnant woman was multigravida.
DISCUSSIONS
The significant difference in IgG seropositivity between cases and controls of present study is in agreement with the studies of Siemer et al., 2008 at Ghana [26] and Jeremiah et al., 2011 at Nigeria [27] who also found statistically significant difference between the IgG seroprevalence rate of infertile and pregnant women (P < .001). Similar to the present study, Sharif et al., 2011 in Saudi Arabia also found no statistically significant difference in the IgA seroprevalence rates of cases and controls (25% vs 10%, P = .4) [28]. But, in contrary to the present study statistically significant difference was present in the IgA seroprevalence rate of infertile and pregnant women in the study of Siemer et al., 2008 (14% vs 3%, P < .001) [26].
The use of Nucleic acid diagnostic techniques such as polymerase chain reaction (PCR) has revolutionized our ability to diagnose almost all the microbes including genital tract Chlamydia trachomatis infection in minimum time with stringent specificity. Sensitivity and specificity of this test on FVU sample have been proven comparable to those obtained on samples collected directly from cervix or urethra [26]. Moreover, FVU sample collection is noninvasive, more acceptable to patients and does not require help of medical personnel to perform vaginal speculum examination which is needed to collect endo-cervical swabs. Sensitivity and specificity of PCR on urine samples are 87% and 99.8% respectively [29]. The lower PCR positivity rate and non-significant difference between infertile and pregnant groups is in agreement with several previous studies. Siemeret al., 2008 conducted a case control study in Ghana among 191 infertile and 248 pregnant women. PCR testing of FVU samples could not reveal any significant difference between the 2 groups (2.4% vs 1.6%, P> .05) [26]. Ramahi et al., 2008 at Jordan also found no significant difference (P> .05) in PCR positivity tested on endocervical swab of 152 infertile (3.9%) and 146 pregnant (07%) women [30]. In another case control study of Muvunyi et al., 2011 at Rwanda, 303 infertile and 312 fertile women were investigated. PCR testing on vaginal swabs were performed. The PCR prevalence was relatively low and did not differ significantly between the 2 groups (3.3% vs 3.8%, P> .05) [31]. But in contrary to the present study, Pramanik et al., 2012 at Mumbai, India could find significant difference in the PCR positivity rate between infertile and pregnant women (P< 0.0005) [32].
The present study demonstrated that sensitivity was higher with R1 – R2 primer than MOMP primers. It is in contrary to the study of Mahony et al., 1993, in which they found that the sensitivity of MOMP based PCR assay was better than rRNA DNA based PCR [23]. 16S ribosomal RNA genes contain highly conserved stretches of nucleotide sequences in a large group of microorganism. It is genus specific and more than 95% identical in Chlamydia trachomatis, Chlmydia psittaci and Chlamydia pneumoniae [24]. So PCR with rRNA DNA is less specific than PCR assay targeting MOMP primer. But, in the present study, the pregnant woman (P6) who gave amplified products with R1-R2 primer only was also IgA seropositive and IgG seronegative. Serum IgA is an indicator of active infection. The patient also had history of white discharge, dysmenorrhoea, chronic pelvic pain, menorrhagia and history of urethral discharge in partner suggesting presence of current sexually transmitted infection. So to conclude, the patient was currently infected with Chlamydia trachomatis. One major problem with PCR is the presence of potential inhibitors in clinical specimens that can lead to false negative results. Genital tract and urine specimens are known to contain several factors that inhibit DNA polymerase and the exact nature of all of the inhibitors remains to be defined [33].
When individuals acquire Chlamydial infection, there is a lag period/ time interval before antibody response. Similarly antibodies persist for a long time after an infection that is resolved by cellular immune response [33]. In the present study and also in the above mentioned studies IgG positivity was relatively higher than PCR. While serological tests cannot replace the sensitive and specific direct tests, they may be useful in identifying Chlamydial etiology in ascending upper genital tract infection, where direct tests may often fail to detect the presence of organism. As, chronic / persistent infection will induce an immune response and inflammatory reactions resulting in a cyclic process of scarring of the infected tissue leading to partial or total obliteration of the fallopian tubes causing tubal factor infertility or sub infertility [4, 12, 17] persistence of serum antibodies are better predictors of infertility and a negative urine sample cannot exclude infection of upper genital tract infection. This corroborates with the study of Joyee et al., 2007 in Chennai, India, who also could not find any correlation between IgG positivity detected by immune-peroxidase kit and PCR from genital swabs in STD patients [34].
Based on the results of ELISA and PCR the proportion of this infection among all the study participants was 8.75%, and among the infertile population was 15% in the present study. It was comparable to the cross sectional study of Pramanik et al., 2012 at Mumbai in India. The average infection rate was 12.1%, highest in women with infertility (18.6%) or with ectopic pregnancy (25%). They used PCR to evaluate current infection and ELISA for IgG antibody against Chlamydia trachomatis to detect past infection. In contrary to the present study statistical analysis revealed significant association between current C. trachomatis infection with infertility when comparing infected fertile (18.6% vs. 9.4%, odds ratio: 2.19, P <.0005) and uninfected infertile women (45.6% vs. 27.3%, odds ratio: 2.24, P<.0001). They excluded women positive for C. trachomatis antibody from analysis as presence of C. trachomatis antibody is known to be associated with tubal factor infertility [32]. In another study Pratibha et al., 2010 in Chidambaram found much higher seroprevalence (62%) in infertile women. Infection was found in 56% of primary infertility cases and 73% of secondary infertility cases [35]. From the literature, it is clearly evident that prevalence was higher in African countries [26, 27, 36] than South East Asian countries [19, 28, 30, 32]. According to WHO prevalence estimates there is vast difference in the prevalence in different geographical regions. 3.89 % females are infected in WHO African region, whereas only 1.09% females are infected in WHO South East Asian region in the year 2005 [1]. As in the present study infertile population is taken, the prevalence is higher than the general estimates. There is variation in the contribution of previous history of STDs with infertility. It has been considered lower among infertile population of Asia than Africa in different studies [37]. In the present study 13.33% of primary infertile women and 20.00% of secondary infertile women were infected. There was no statistically significant difference in the magnitude of infection between the 2 groups (P = .6287, OR = 0.6154, 95% CI 0.09449 to 4.008). Malik et al., 2006 in Aligarh found that Chlamydial positivity detected by endo-cervical swab culture and antigen detection was seen in 27% of women with primary infertility and 30.6% with secondary infertility. Though the prevalence was much higher, still there was no statistically significant difference between the proportions (P = >.05) [19]. But in a community based study carried out in Saudi Arabia, Kamel Remah M, in 2013 found statistically significant (P = .0096) higher prevalence of infection among primary (11.72%) than secondary (3.28%) infertile women [38]. Similar to the present study prevalence of infection was 13.33% among primary infertile women in the study of Deshmukh et al., 2013 in Maharashtra, India. But they also observed a statistically significant difference when C. trachomatis IgG positive patients were compared in respect to primary vs secondary infertility (X2 -10.44 P < .05) [39].
CONCLUSION
The proportion of Chlamydia trachomatis seropositivity (IgG and IgA) was higher in infertile women than pregnant women, though there was no significant difference in PCR positivity between the 2 groups. So, persistent C. trachomatis infection must be recognized as a risk factor of infertility. The low PCR positivity in FVU sample further helps to conclude the diagnostic utility of serological tests in screening of infertile women.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
The authors sincerely acknowledge the contribution of all the staffs of the Department of Microbiology, R. G. Kar Medical College, Kolkata and Department of Biochemistry, Institute of Post Graduate Medical Education & Research, Kolkata.

