All published articles of this journal are available on ScienceDirect.

An Epidemiological Review on Emerging and Re-Emerging Parasitic Infectious Diseases in Malaysia
Abstract
Emerging infectious diseases are infections that have recently appeared in a population over a defined period of time whereas, re-emerging infectious diseases are those that were once a health problem in a particular region or a country and are now emerging again. Parasitic infectious diseases represent a serious health problem in many developing countries and recently have started spreading to developed nations via international traveling or immigration. Malaysia is facing many challenges caused by various parasitic pathogens. The lack of awareness among disadvantaged populations such as the Orang Asli community and the dependency on foreign workers has led to an influx of immigrants to Malaysia from countries endemic to various parasitic diseases. Understanding the social and economic dynamics of such diseases can help anticipate and subsequently control their emergence. Raising public awareness, developing robust public health infrastructure and implementing point-of-care diagnostics will help curb the spread of such diseases. This review provides epidemiological insights into the reported emerging and re-emerging parasitic infectious diseases in Malaysia over the past two decades.
1. INTRODUCTION
Emerging infectious diseases are infections that have recently appeared in a population over a defined period of time whereas re-emerging infectious diseases are those that were once a health problem in a particular region or a country and now are emerging again [1]. The World Health Organization (WHO) defines zoonoses infections transmitted from animals to humans with wild animals as the source of most emerging infections [2]. Countries in Southeast Asia have witnessed an increase in the incidence of some parasitic infectious diseases in recent decades [3]. Malaysia is facing many challenges caused by various parasitic pathogens. The lack of awareness among disadvantaged populations such as the Orang Asli (i.e. indigenous people of Peninsular Malaysia) and the dependency on foreign workers have led to an influx of immigrants to Malaysia from countries endemic to various parasitic diseases [4]. Moreover, the constant disturbance of natural habitats by humans have led to a loss of biodiversity which has led to an increase in the prevalence of infectious diseases [5]. Furthermore, foodborne and waterborne diseases such as, intestinal protozoan infections that are associated with poor hygiene, are still a health problem in Malaysia, particularly among rural communities. Understanding the dynamics of parasitic infections can help anticipate and subsequently control their emergence and re-emergence. There is no readily available vaccine for most parasitic infections, therefore, developing robust healthcare infrastructure, implementing point-of-care diagnostics as well as raising awareness on hygienic practices are essential tools to curb the spread of such infections [3]. This review provides epidemiological insights into the reported emerging and re-emerging parasitic infectious diseases in Malaysia over the past two decades.
2. EMERGING AND RE-EMERGING PARASITIC INFECTIOUS DISEASES
Parasitic diseases are generally grouped into human and animal diseases. However, zoonotic infections fall into both categories as they can infect humans as well as animals [6]. The following are some of the important parasitic infectious diseases that have been emerging and/or re-emerging in Malaysia arranged in alphabetical order:
2.1. Amoebiasis
Amoebiasis is an emerging parasitic infectious disease with significant morbidity and mortality, particularly in poor tropical regions. Infection is acquired by ingesting food and/or water contaminated with the parasite Entamoeba histolytica [7]. A large number of hospital-based studies in Malaysia has been carried out with the aim to determine the prevalence of amoebiasis [8]. A study was conducted from 2005 to 2006 with the aim to determine the prevalence of gastrointestinal protozoan parasites in Kota Kinabalu, Sabah. It was concluded the parasitic load of Entamoeba histolytica was the highest and that the school environment was the potential medium to spread infections. In a study conducted to detect the true prevalence of E. histolytica, E. dispar and E. moshkovskii infections among Orang Asli tribes in western Malaysia [9], the results showed that most individuals were infected with E. dispar (13.4%), followed by E. histolytica (3.2%) and E. moshkovskii (1.0%) with a low prevalence of mixed infections [9]. This has provided new insight into the distribution of amoebiasis among these underprivileged communities. A cross-sectional study was conducted in 2014 to investigate the intestinal risk factors of polyparasitism among school children in Pahang (the third largest Malaysian state by area) [10]. Their results showed that Entamoeba spp. infections had a low prevalence compared to infections with other parasites such as Trichuris spp. and Ascaris spp. [10]. Although amoebiasis is mainly encountered in poor rural areas in Malaysia, it has the potential to be transmitted and thus emerges among urban populations. In developed countries, amebiasis is slowly emerging among returning travelers and men who have sex with men (MSM) [11]. Although molecular-based diagnostic methods such as the Polymerase Chain Reaction (PCR) are readily available, they remain underutilized aiding in the misdiagnosis of this infection [11]. There is no available vaccine against any Entamoeba spp. infection yet, therefore, establishing robust healthcare infrastructure particularly in remote villages, implementing point of care diagnostics as well as raising awareness on the importance of hygienic practices are essential tools to curb the spread of amoebiasis.
2.2. Ascariasis
Ascariasis is a re-emerging infectious disease caused by an infection with the large roundworm, Soil-Transmitted Helminth (STH) Ascaris lumbricoides [12]. It is one of the most common infections affecting travelers and is grouped under neglected Intestinal Parasitic Infections (IPIs). Southeast Asia accounts for a large number of Ascaris cases with 126 million infected individuals [13]. Malaysia has not been spared from the burden of Ascariasis particularly among poor communities such as the Orang Asil. In 1988, the status of helminth infections among children living in the slum areas of Kuala Lumpur was assessed with 50% of these infections due to Ascaris lumbricoides [14]. This indicated that the frequency of Ascaris lumbricoides infections were age-dependent suggesting lower incidences in infants than in older children [14].
The prevalence of parasitic infections among aboriginal children in the state of Kelantan was assessed in 1996 with Ascaris lumbricoides being detected in 79.8% of stool samples. In 2003, a study was conducted to determine the prevalence of parasitic infections caused by Entamoeba histolytica, Ent-amoeha coli, Giardia lamblia, Ascaris lumbricoides, and Trichuris trichiura among schoolchildren living in the Crocker Range Park (CRP) of the state of Sabah [15]. Results showed that Trichuris trichiura infection was the highest (10.0%) compared to Ascaris (8.7%) and hookworm (3.3%) with a 12.6% prevalence for a single infection, 4.6% of double infection and 2.0% of triple infection [15]. In 2016, a cross-sectional study was conducted on 388 migrant workers in Malaysia from various working sectors to detect the prevalence of intestinal parasitic infections [16]. Results showed that Ascaris lumbricoides occurred in 72.8% of the Nepalese workers and 68.1% on the Indian workers. This indicated that environmental and socio-demographic factors played a major role and that workers who stayed in Malaysia for less than a year were most likely to show high levels of infection [16]. A year later in 2017, a study reported that 62.9% of migrant workers were positive for at least one intestinal parasite within one year of their arrival in Malaysia with A. lumbricoides being the highest (43.3%) in prevalence [17]. Routine mass-drug administration on newly arriving foreign workers and health education programmes on the importance of personal hygiene and sanitation are needed in order to minimize the incidence of ascariasis and prevent its re-emergence. As the number of immigrant workers in Malaysia has drastically increased over the last decade, there is an urgent need for reliable epidemiological data of parasitic infectious diseases. Moreover, ascariasis along with other STHs is transmitted via the fecal-oral route as a result of poor sanitary practices. Therefore, detecting the prevalence, identifying risk factors and raising awareness are key elements to curb the spread of this disease.
2.3. Blastocystis
Blastocystis is an emerging zoonotic disease caused by the intestinal protozoan Blastocytis hominis. Poor hygiene and sanitation are major risk factors for its spread. It affected mostly children, animal handlers, travelers, immigrants as well as soldiers posted in endemic countries [18]. Blastocystis is not yet endemic in Malaysia, however, there are sporadic high numbers of cases reported and with the heavy influx of immigrants from neighboring countries, this can lead it to become endemic. The recent increase in the number of reported blastocystis cases can be attributed to the advancement in diagnostic methods [19]. In 2004, a cross-sectional survey among three Orang Asli tribes provided important epidemiological data of Blastocystis infection revealing that untreated drinking water was the main source of blastocystis transmission which raised the need for an intervention strategy to practice good water treatment in order to reduce the incidence of blastocystis [20]. In 2011, blastocystis was reported in the water of two rivers located in recreational areas in Malaysia. Such detection indicated that the causal parasite Blastocystis hominis has the potential to be easily transmitted to humans [21]. In 2012, the prevalence of blastocystis among school children living in rural areas of the state of Pahang was assessed [22]. Their results showed that blastocystis was high among children and that infected drinking water was the main source of infection which required raising awareness among the affected children as well as their parents [22]. Zoonotic transmission of Blastocystis sp. from livestock was investigated in different Malaysian farms and results showed that the proximity to human dwellings accounted for the multiple infections [23]. In 2016, a cross-sectional study was carried out to investigate the incidence of intestinal parasitic infections among children from five states in Peninsular Malaysia [24]. Their results showed that the blastocystis was the most prevalent with 10.6% which was attributed to the lack of education among these rural communities [24]. It is worth mentioning that blastocystis cysts are resistant to chlorination which allows them to persist for longer times in the environment [25]. Moreover, the ingestion of only a few cysts is enough to cause infection [26]. Therefore, local authorities must implement strategies that provide better health facilities related to water treatment to avoid the emergence of blastocystis in Malaysia.
2.4. Cryptosporidiosis
Cryptosporidiosis is an emerging zoonotic parasitic disease that spreads via contaminated food and water and is caused by the enteric parasite Cryptosporidium parvum. Infection is acquired by ingesting water or food contaminated with the oocysts of Cryptosporidium species which in some cases can be fatal [27]. In 2007, a study was conducted to re-evaluate the occurrence of Cryptosporidium species in the fecal samples of birds in the national Malaysian (Zoo Negara) [28]. Based on their results, an association of cryptosporidiosis among the affected birds and their handlers was established indicating a zoonotic transmission [28]. In 2007, a cross-sectional study was conducted among Orang Asli communities in the state of Pahang to investigate the distribution of both Cryptosporidium and Giardia species [29]. Results showed that cryptosporidiosis had a prevalence of 4.1% with no gender bias between Cryptosporidium and Giardia spp. indicating that such diseases remain significant health problems among the Orang Asli in Malaysia [29]. In 2012, a study was conducted to detect the prevalence of cryptosporidiosis in 130 diarrheal stool samples of children at two urban hospitals in the state Selangor [30]. Their results indicated that 4.62% of samples were positive for Cryptosporidium spp. indicating that hygiene standards should be improved and monitored in daycare centers where many parents leave their children for long hours [30]. In 2017, a cross-sectional study was conducted on 388 migrant workers in Peninsular Malaysia to determine the status of protozoan infections [31]. Microscopy examination showed 42 (10.8%) positive with Giardia spp. and 12 (3.1%) samples with Cryptosporidium spp. which highlighted the potential risks of waterborne as well as foodborne infections in the spread of such infections [31]. Cryptosporidiosis has the potential to spread and emerge as a significant health problem in many rural areas across Malaysia. It can become life-threatening particularly among the elderly, small children and AIDS patient. Therefore, regular monitoring of water and food sources using investigational methods such as Microbial Source Tracking (MST) can distinguish between the human and animal sources of fecal contamination hence preventing its emergence [32].
2.5. Filariasis
Lymphatic Filariasis (LF), also known as Elephantiasis, is a re-emerging parasitic infectious disease caused by the nematode worms Wuchereria bancrofti, Brugia malayi and Brugia timori that are transmitted to humans by the bite of infected Anopheles, Culex and Aedes mosquitoes. Brugia malayi is the main parasitic species that causes LF in Malaysia [33]. Between 2003 and 2006, five patients with clinical manifestations of LF were referred to the University Malaya Medical Centre [34]. Results showed that two of the patients tested positive with an unknown animal filarial worm named Brugia pahangi [34]. It was later reported that domestic cats in the suburbia, where all patients came being tested positive for Wuchereria bancrofti microfilaria (mf) even though there was no recorded history of Brugia malayi infection in the area, can be the source of zoonotic infection. Despite the fact that Mass Drug Administration (MDA) programmes have been successfully executed in Malaysia as part of the Global Program to Eliminate Lymphatic Filariasis (GPELF) by the year 2020 [35], Malaysia continues to face challenges of acquiring the disease due to the arrival of immigrant workers as well as the vector’s natural presence [36]. In 2017, Wuchereria bancrofti infections were reported among foreign immigrants coming to Malaysia [17] outnumbering Brugia malayi infections [23]. The recent influx of foreign workers from LF endemic countries is a matter of concern in Malaysia as it can lead to its re-emergence [37]. Moreover, the unavailability of reliable diagnostic tests is another obstacle in the implementation of elimination programmes in areas where brugian filariasis is endemic. Regions that used the Brugia Rapid (BR) diagnostic test, developed earlier in Malaysia to detect IgG4 antibodies, recorded a sharp fall in mf positive rates [38]. BR would be very useful as a diagnostic tool to aid in the mapping and certification phases of the filariasis elimination programme in brugian filariasis endemic areas [39].
Although Malaysia is considered endemic for LF, the disease is generally controlled as a result of the successful MDA program. However, LF has the potential to re-emerge mainly due to its easy mode of transmission through blood-sucking mosquitoes as well as the presence of a large number of immigrant workers in Malaysia arriving mostly from LF endemic countries. The ministry of health, as well as other organizations, must play a role in raising public awareness to improve knowledge of the diseases and increase the chances to take part in the MDA program.
2.6. Giardiasis
Giardiasis is an emerging parasitic infectious disease that represents a significant public health burden causing diarrhoeal diseases particularly in tropical countries [40]. Despite great advances in the socioeconomic status of Malaysia, intestinal parasitic infections coupled with malnutrition are still a problem mainly among Orang Asli children in poor rural areas [41]. In 1998, a study was conducted to investigate the prevalence and risk factors of Giardia duodenalis infection among 917 individuals aged between 2-70 years old in Malaysian rural communities [42]. Their results showed that 19.2% of individuals were infected with G. duodenalis and that person-to-person contact was the main mode of transmission [42]. Good hygiene, as well as awareness, can control Giardiasis among such communities. In 2005, a cross-sectional study investigated Giardiasis as a predictor of childhood malnutrition among Orang Asli children in the state of Selangor [43]. Results showed that Giardia duodenalis was detected in 24.9% of children indicating that Giardiasis was indeed considered as a predictor of malnutrition among such population [43]. In 2011, the distribution of waterborne parasites was investigated in both Peninsular Malaysia and the southeastern coast of Thailand [44]. Results showed that the water was more contaminated with Giardia cysts and Cryptosporidium oocysts compared to those in Thailand [44]. It has been reported that Malaysian waters and soil are generally contaminated enough to act as vehicles to transmit Giardiasis [45]. Giardia spp. is considered an opportunistic pathogen among HIV/AIDS patients. Therefore, investigating its prevalence and epidemiology can help to curb its emergence practically in the midst of a rise in HIV cases in Malaysia [46]. In 2011, a study was conducted to examine stools specimens from 122 patients with HIV/AIDS. Results revealed that the zoonotically important Giardia duodenalis was the identified species [46]. More studies are needed to analyze this pathogen not only in humans but also in domestic and wild animals in Malaysia [46]. In 2012, a study on Giardiasis among Malaysian Orang Asli tribes have identified Giardia intestinalis as a risk factor [47]. Screening and treating of affected individuals can help health authorities to combat such infection particularly among Orang Asli communities [47]. In 2013, aboriginal children in some Malaysian rural areas were the subject to investigate the burden of Giardia duodenalis infection [40]. Results showed that there was a strong association between such infection and the weight of affected children indicating that more efforts from the local health authorities are required to identify and implement control measures among communities [40]. The first study in Malaysia to molecularly characterize Giardia duodenalis infection in 310 goat fecal specimens was conducted in 2013 [48]. Their results revealed that detecting the ‘zoonotic’ assemblages A and B indicates that these infected goats can act as potential reservoirs for human Giardiasis [48]. In order to prevent the emergence of Giardiasis in Malaysia, a multidisciplinary approach is required to determine the level of water contamination with Giardia, Cryptosporidium and other zoonotic parasites [45].
2.7. Malaria
Malaria is the most important emerging parasitic disease worldwide. It is caused by the Plasmodium spp. and is transmitted to humans through the bite of infected Anopheles mosquitoes. Malaria has reached alarming levels in some parts of the world mainly due to the emergence of drug-resistant parasites as well as insecticide-resistant vectors [18]. Malaysia is facing tremendous challenges in regard to the increasing incidence and disease burden of urban malaria due to unplanned development around large cities. One of such challenges is that the parasites Plasmodium falciparum and Plasmodium vivax is naturally found in all of the Association of Southeast Asian Nations (ASEAN). Although Malaysia had successfully controlled the spread of both Plasmodium falciparum and Plasmodium vivax, it seems that the incidence of Plasmodium malariae and Plasmodium knowlesi has significantly increased over the past decade [49]. Plasmodium knowlesi, also known as the fifth human malaria parasite, is naturally found in long-tailed and pig-tailed macaques [50]. During an emerging zoonosis, significant mutations that occur in prokaryotic pathogens can be traced. However, when it comes to eukaryotic parasites, there are many challenges faced [51]. It is now known that both P. falciparum and P. vivax have been endemic for many years [51]. In contrast, P. knowlesi infections were rarely detected in humans only until recently when a large number of cases started to be reported in the states of Sabah and Sarawak [52]. P. knowlesi is now a major cause of human malaria in Malaysia particularly in these two states threatening the progress of control programs. The first case of human knowlesi malaria was reported from Peninsular Malaysia back in 1965 [53] followed by a second case a few years later [54]. However, large numbers of human infections began to be reported in the state of Sarawak in the early 2000s [55]. Ever since, P. knowlesi has become the major cause of human malaria across the states of Sabah and Sarawak [56, 57]. Despite the success of malaria control programs in Malaysia, Plasmodium knowlesi has emerged as a zoonotic species and a large number of cases were first reported in 2004 in Sarawak [49] followed by Peninsular Malaysia later on [50, 58]. In recent years, the epidemiology of malaria is becoming more complex in Malaysia. There is a shift towards infections among men and adults rather than women and children [59]. This can be attributed to the fact that men are engaged in more outdoors activates such as plantation and forest works exposing them to the bites of infected vectors [60].
There are many factors that contribute to the emergence of P. knowlesi malaria in Malaysia. In 2009, the highest percentage of P. knowlesi malaria was reported to be 87% at the Kudat district hospital in the state of Sabah [56]. In 2013, an increase in the prevalence of P. knowlesi in Sabah was reported [61] as a result of significant deforestation that led to the increased exposure to the arthropod vectors [61]. Such activities have also led to vector behavioral changes as seen in the Kinabatangan region where Anopheles Donaldi replaced the previously dominant Anopheles Balabacensis [62]. In 2015, Plasmodium knowlesi was reported in humans as an admixture of two highly divergent parasite populations, each associated with different macaque reservoir host species [63]. Moreover, the resistance of the Plasmodium spp. to antimalarial drugs has led to great difficulties in managing the disease. Furthermore, what makes the diagnosis of P. knowlesi difficult is that microscopically it is indistinguishable from P. malariae [61]. Therefore, the ministry of health of Malaysia along with academic and research institutes should increase their effort to raise public awareness as well as implement the use of point-of-care molecular techniques to characterize mixed infections amongst which most of them go misinterpreted or underreported and thus preventing their emergence.
2.8. Toxoplasmosis
Toxoplasmosis is a re-emerging parasitic infectious disease caused by a protozoa Toxoplasma gondii [64] that continues to be an important cause of morbidity in the tropics. The prevalence of Toxoplasmosis in Malaysia has significantly increased in the last three decades. In 1983, a study was conducted at the Ophthalmology Clinic in Universiti Kebangsaan Malaysia (UKM)reported 31 cases of ocular Toxoplasmosis [65]. Studies have shown that Malays have the highest incidence of toxoplasmosis followed by Indians and Chinese [65]. One of the common risk factors to acquire a Toxoplasma infection is the direct contact with infected cats, consumption of uncooked meat and less commonly through blood product or organ transplantation [64]. Early studies on the seroprevalence of toxoplasmosis in Malaysian pregnant women estimated it to be 27.4% [66] however there has been a significant increase in the percentage of this disease in this group of the population as of 1990 onwards [67]. Moreover, toxoplasmosis was found to be directly associated with abortions and stillbirths [64]. There has been a high prevalence of toxoplasmosis in Malaysia among HIV/AIDS individuals [64]. In 2003, a total of 301 serum specimens of HIV/AIDS patients were tested for anti-Toxoplasma IgG antibody by ELISA [68]. Results showed that the seroprevalence was 41.2% with a higher percentage among the Malays in the Malay, Chinese than Indians [68]. From 2007 to 2010, a study evaluated the seroprevalence of Toxoplasma gondii among 495 Orang Asli living in Peninsular Malaysia with an overall seroprevalence of 37.0% [69]. Given the high prevalence of toxoplasmosis among Orang Asli pregnant women, health surveillance programs in such communities should start early during the antenatal routine check-up [70]. In 2017, the seroprevalence of Toxoplasma gondii among migrant workers in Peninsular Malaysia was evaluated [71]. Their results showed that there was an increased prevalence of 57.4% compared to previous reports [72]. Southeast Asia including Malaysia harbors a large variety of ecological niches that favor the spread and transmission of Toxoplasma spp. and with the rapid development that is happening in the region, the incidence of toxoplasmosis might be on the rise in Malaysia leading to its re-emergence. Therefore, surveillance programs should be initiated to facilitate early diagnosis and treatment [69]. Moreover, the role of domestic cats and environmental contamination with Toxoplasma oocyst must be addressed in order to implement preventative measures.
2.9. Trypanosomiasis
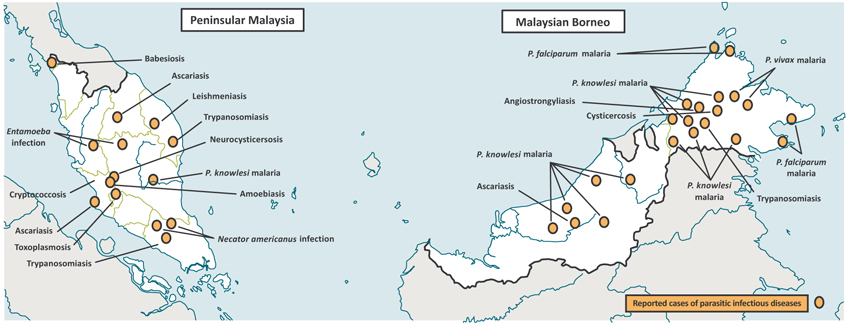
Trypanosomiasis or Human African Trypanosomiasis (HAT) is an emerging vector-borne parasitic infectious disease caused by infection with protozoan the parasite Trypanosoma species. They are transmitted to humans by tsetse fly bites which have acquired their infection from human beings or from animals harboring human pathogenic parasites [73]. Animal trypanosomiasis existed in Malaysia for many decades as it was reported in cattle and horse. Malaysia is considered endemic for animal trypanosomiasis caused by Trypanosoma evansi [74]. In 1996, it was reported that trypanosomiasis in the cattle caused significant losses in milk production and body weight [75] and that stable flies, as well as horse flies, can transmit Trypanosoma evansi in Malaysian cattle [76]. Deer farming has become popular in Malaysia recently and there is a potential for trypanosomiasis to occur in farmed deer. In 2007, a livestock deer breeding center located in the state of Perak was the place to investigate an outbreak as well as the seroprevalence of Trypanosoma evansi [77]. Although human trypanosomiasis is not yet considered a health problem in Southeast Asia including Malaysia [78], but cross-species zoonosis from local infected animals [79]. The existence of human trypanosomiasis from neighboring Thailand, reporting cases of trypanosomiasis in cattle from neighboring Indonesia, can all lead to its emergence. Therefore, improving diagnostic tests, awareness, and field investigations can aid to detect both human and animal cases (Fig. 1).
3. FACTORS INFLUENCING EMERGENCE OF INFECTIOUS DISEASE
There are many factors that influence the emergence and re-emergence of parasitic infectious diseases in Malaysia; those include the displacement of human populations due to natural disasters, deliberate changes in biodiversity due to deforestation, influx of immigrant foreign workers from endemic countries, poor hygienic practices, lack of proper healthcare infrastructure in some rural areas, as well as some local food habits [6]. Some of these factors will be discussed as follows:
3.1. Displacement of Human Populations
The mass movement of human populations from their homes or relocating them in temporary refugee camps as seen during floods is a serious problem in Malaysia particularly during the monsoon season [6]. This sudden displacement of population adversely affects the safe disposal of human excreta and often destroys drainage systems leading to direct exposure to many intestinal parasites as well as their potential vectors. One of the worst floods to hit Malaysia occurred in the city of Kota Bharu of the state Kelantan back in 2014 when approximately 104,000 people were displaced from their homes exposing them to many diseases. Luckily and with great efforts by many volunteers, the situation was handled with efficient distribution of aid .
More recently in 2018, two lives were claimed and nearly 12,000 people were evacuated from their homes in the state of Pahang [80]. It was reported by Malaysia's disaster management agency that the flood victims were sheltered at relief centers in the states of Johor, Terengganu, Pahang, and Sabah. It was learned later that the flood was mainly due to the continuous downpour and the inability of drains in those places to accommodate such water flow. Therefore, more efforts from states and federal governments are required to improve the drainage systems in such areas.
3.2. Deliberate Changes in Biodiversity
Biodiversity is defined as the variability among terrestrial, marine and aquatic living organisms [81]. For many zoonotic parasites, direct exposure with wildlife reservoirs and vectors is a major risk factor [82] leading to what is termed as ‘host-jumping’ where an animal parasite infects humans due to activities occurring in proximity to wildlife areas [81]. Malaysia has witnessed rapid development over the past three decades in terms of urbanization, deforestation and road construction. Such activities have subsequently led to deforestation as well as changing the ecosystem of some of the animals and insects that are potential vectors for many parasitic infectious diseases [83]. Such urbanization has allowed some parasitic infections to significantly increase from isolated rural areas to larger communities. As a consequence, this emerging infection (disease) will spread even further among the population through the use of modern transportation [1]. Displacement of wildlife can also result in global warming which subsequently can lead to the spread of infections to human populations [84]. For example, land changes due to the construction of residential and retail buildings in Malaysia can cause habitat destruction, fragmentation as well as local species extinction which in turn contribute to the loss of biodiversity [81]. Therefore local authorities along with the developers must properly plan the use of land to prevent exposure or drastic changes to wildlife hence preventing the emergence and re-emergence of parasitic diseases.
3.3. Influx of Immigrant Foreign Workers
The stable growing economic conditions in Malaysia seem to encourage the movement of large numbers of immigrant workers, those coming from endemic areas with various parasitic infectious diseases [1]. Malaysia is always lacking unskilled labor hence it attracts migrants to sustain its economic development. Accordingly to the Malaysian home ministry, there are more than 1.7 million foreign workers in Malaysia as of June 2017 and majority from Indonesia [85]. The presence of such large numbers of foreigners is a major healthcare concern for Malaysia. Such concern is reflected upon formulating health policies. The problem in monitoring emerging and re-emerging parasitic diseases is that advanced surveillance and monitoring systems are readily available in developed nations rather than developing countries that are directly affected by such diseases [86]. Priority should be given to set up 'smart surveillance' measures in hotspots across Malaysia.
4. DISCUSSION
All of the factors discussed above along with the ongoing evolution of microbial variants and drug resistance contribute in one way or another in putting Malaysian people at risk of being infected or affected by one or more of these emerging and re-emerging parasitic diseases. It seems that such diseases will continue to appear leading to unpredictable outbreaks or epidemics that challenge healthcare personnel and emphasize the urgent need for effective surveillance and control measures. Despite the challenges faced, Malaysia is strongly committed to curb the spread of these diseases. One good example is the ‘food handlers’ training programme’ adopted by the Ministry of Health in Malaysia in 1996 to ensure hygienic practices during handling, preparation and sale of food and prevent the spread of food-borne diseases [87]. Moreover, Malaysia has established indicator-based and event-based surveillance systems as well as a web-based early outbreak reporting system called e-wabak which has the potential to include all hazards. Orang Asli in rural Malaysia is by far the most vulnerable population to polyparasitism [10]. There is an urgent need to improve the quality of life of Orang Asli and implement awareness programmes to reduce the incidence of such disease particularly among children [10]. Preserving wildlife should be taken into consideration in the risk analysis framework to prevent zoonoses [88]. More research is needed to investigate the epidemiology of zoonoses in Malaysia as well as improve and implement the use of point-of-care diagnostic tools particularly in the remote and rural areas [88]. The way forward for Malaysia to reduce the risk of emerging and re-emerging parasitic diseases is through the scope of World Health Organization (WHO) International Health Regulations (IHR) 2005 and OIE Terrestrial Animal Health Code 2011 with the ‘One Health’ approach to collaboration. Updating epidemiological databases will help characterize host-pathogen interactions and provide a better understanding of disease dynamics. Last but not least, health education and health awareness across the nation go a long way in enhancing prevention and awareness among the general public on intestinal parasitic infections.
CONCLUSION
The lack of awareness, poor hygienic practices among socioeconomically disadvantaged communities and the rapid influx of immigrant workers are major factors that contribute to the emergence and re-emergence of parasitic infectious diseases in Malaysia. Therefore, raising public awareness, developing robust public health infrastructure and implementing point-of-care diagnostics will help curb the spread of such diseases not only in Malaysia but in Southeast Asia as well.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The authors confirm that the data supporting the findings of this study are available within the article [10] at [10.1371/ journal.pntd.0003074], article [87] at [10.1016/j.foodcont.2010 .12.011], and article [88] at [10.3201/ eid1012.040707].
FUNDING
The authors would like to thank the research management center at MAHSA University for providing us with the finical support through the research grant (RP68-09/14) to conduct this review.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank the management of MAHSA University, the Dean of the Faculty of Medicine & Biomedical Sciences and the Head of Department of Microbiology/ Parasitology for their support in providing all the logistics, assistance, and guidance needed to write this review.

