All published articles of this journal are available on ScienceDirect.

SARS-CoV-2 Invasion: What Happens to Other Respiratory Viruses?
Abstract
This letter briefly presents the relationships between respiratory viruses in the years prior to and during the COVID-19 pandemic. Viral common colds are self-limiting infections that typically resolve within a few days. However, when well-established epidemiological relationships are disrupted during a pandemic, they behave differently. For instance, during the 2009 influenza pandemic, while the majority of seasonal respiratory viruses lost ground under the pressure of a new pandemic strain, some others (for instance, human rhinoviruses) continued to circulate along with the pandemic pathogen and in some cases, even delayed its spread. With the arrival of the COVID-19 pandemic, the degree of circulation of many respiratory viruses has changed dramatically. Along with a significant reduction in the circulation of many seasonal respiratory pathogens, rhinoviruses, respiratory syncytial virus and non-COVID-19 coronaviruses—being the most frequently identified respiratory pathogens—have shown their unique capability to compete with SARS-CoV-2.
INTRODUCTION
The COVID-19 pandemic highlighted new and unusual relationships between respiratory viruses for the first time. Recently, many publications have appeared on this topic, the analysis of which is necessary in order for the virology community to compare the current situation with situations of past years. This letter briefly discussed the relationships between respiratory viruses in the years before and during the COVID-19 pandemic.
Rhinoviruses, respiratory syncytial viruses, seasonal coronaviruses, adenoviruses, parainfluenza viruses, bocaviruses and metapneumoviruses, among others, are distributed across the globe and are the most frequent cause of the common cold in humans [1]. They are widely considered to be harmless because they are perceived as pathogens only capable of causing mild disease. Among tens and even hundreds of other seasonal respiratory viruses that cause common colds, human coronaviruses (HCoV) known since the 1960s [2] occupy a special place because, taxonomically and structurally, they are closest to SARS-CoV-2 [3]. A list of seasonally circulating HCoV species contains four pathogens belonging to the genus Alphacoronavirus (229E, NL63, HKU1) and genus Betacoronavirus (OC43); they cause self-limiting human infectious diseases that typically resolve within a week [4]. By contrast, in the last 20 years, three highly pathogenic coronaviruses—SARS-CoV-1, MERS-CoV and SARS-CoV-2—have emerged, highlighting the high pandemic potential of the family Coronaviridae, that had previously been considered relatively harmless [5, 6].
Influenza pandemics that occur at intervals of 10-40 years disrupt historically established epidemiological relationships. Seasonal influenza and the common cold—long known to be the most prevalent human infections—have given way to a new pandemic strain [7, 8], the emergence of which was regularly marked by the disappearance of an ancestor of a new offspring drifting in seasonal epidemics. High rates of reduction in non-pandemic respiratory viruses were also detected during the COVID-19 pandemic [9]. However, the relationship between viruses is much more complex and multifaceted than it seems at first glance. Compared to other respiratory viruses, common cold HCoVs are closest taxonomically to SARS-CoV-2 and do not disappear in the same way as the majority of other seasonal respiratory viruses such as influenza. On the other hand, genetically distinct rhinoviruses and respiratory syncytial viruses also co-circulate with SARS-CoV-2 [10].
Interactions between respiratory pathogens in the years prior to and during the COVID-19 pandemic have been highlighted in the literature [11-16]. It has been shown that some viruses can coexist [10] with other respiratory pathogens or compete with them [13]. The spread of some viruses is delayed [10-12, 17-19] or blocked [13] by other viruses.
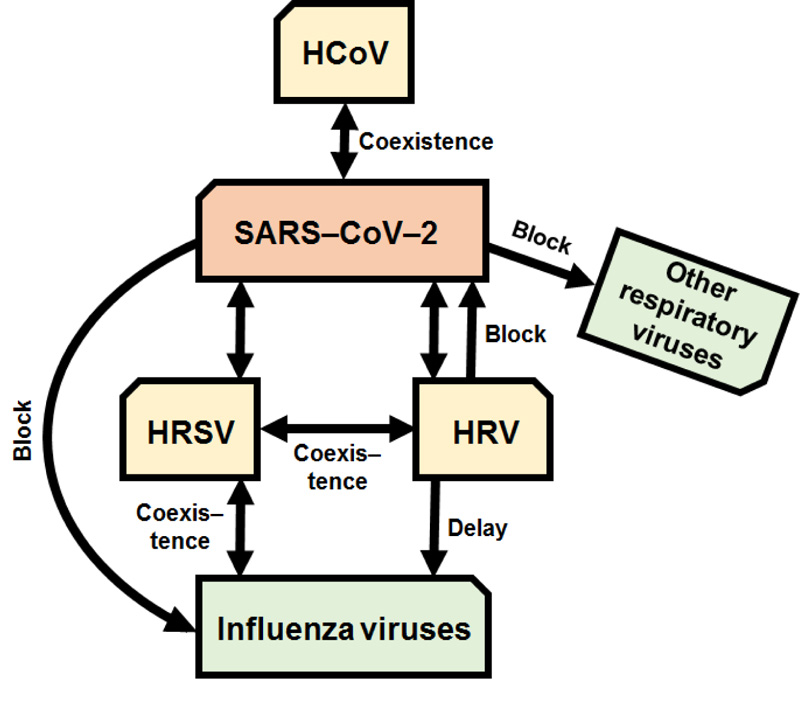
Of greatest interest is the interplay between rhinoviruses, respiratory syncytial viruses, influenza viruses and SARS-CoV-2 that may be manifested in several distinct scenarios (Fig. 1) [10-21].
The spread of influenza A virus—both seasonal and pandemic—might be interrupted by seasonal human rhinovirus [11, 12, 16-18, 21] or blocked by SARS-CoV-2 [19]; in turn, SARS-CoV-2 blocks seasonal influenza viruses [20] but might co-exist with [10, 15] or be blocked [13] by rhinovirus; respiratory syncytial viruses may co-circulate with influenza viruses, rhinoviruses, seasonal human coronaviruses and SARS-CoV-2 [10, 14, 15]. It should be noted that WHO suggests that implementing various hygiene and physical distancing measures may also play a certain role in reducing influenza virus transmission [19].
As an example of the circulation of respiratory viruses during a global spread of SARS-CoV-2, (Fig. 2) displays their distribution in Russia [25]; we believe the situation in one country to be a fair reflection of the general trend of SARS-CoV-2 distribution worldwide [27].
Fig. (2A) schematically represents the central tendency for the distribution of the most common respiratory viruses in the pre-COVID-19 period in some countries of Europe (Italy, UK and Russia), Western Asia (UAE) and East Asia (China) (2012-2016) [10, 22-26]. Of course, in percentage terms, the number of positive respiratory isolates may vary from country to country, from region to region, and from season to season.
Before the COVID-19 pandemic, in 2012-2016, the most frequently detected non-COVID-19 virus was the influenza virus, followed by respiratory syncytial virus and rhinovirus (Fig. 2A). Since the onset of the COVID-19 pandemic, a significant drop in the circulation of non-COVID-19 respiratory viruses compared with previous years has been observed; among these, the most common non-SARS-CoV-2 viruses detected in 2020 were human rhinovirus, HCoV and respiratory syncytial virus (Fig. 2B). Surprisingly, since the end of 2021, a rapid increase in global influenza virus activity has been noted. The majority of influenza viruses detected are H3N2 [19].
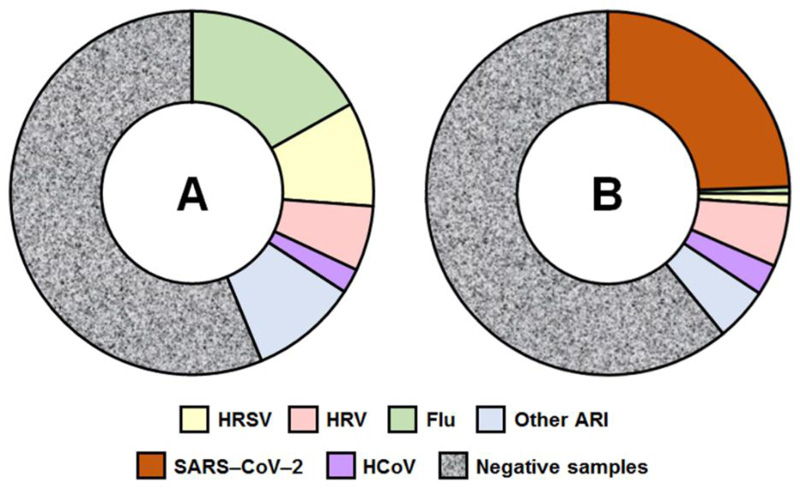
(A) Distribution (%) of respiratory viruses through pre-COVID-19 period (2012-2016) [10, 22-26] and (B) Distribution (%) of respiratory viruses during the COVID-19 pandemic (2020) [25]. Abbreviations: HRSV, human respiratory syncytial virus; HRV, human rhinovirus; HCoV, seasonal human coronavirus other than SARS-CoV-2; flu, influenza viruses types A and B; Other ARI (other viruses caused acute respiratory infections).
CONCLUSION
What allows SARS-CoV-2 to coexist with rhinoviruses and respiratory syncytial virus while displacing other respiratory viruses? The reason may lie in the as-yet-undiscovered delicate molecular mechanisms of infections caused by these agents; finding host factors unique to or common to these viruses could facilitate the development of novel therapeutic approaches to combat the COVID-19 pandemic.
FUNDING
This work was supported by Russian Science Foundation, Grant Number 21-75-30003.
CONFLICT OF INTEREST
Dr. Irina Kiseleva is the Editor-in-Chief of the journal TOMICROJ.
ACKNOWLEDGEMENTS
Declared none.

