All published articles of this journal are available on ScienceDirect.

Viral Molecular Testing of Cerebrospinal Fluid in Adults with Suspected Central Nervous System Infection in an Italian University Hospital Laboratory: A Retrospective Study on 1462 Consecutive Patients
Authors Info & Affiliations
Abstract
Background:
Generally, about half of the patients with central nervous system infections cases remain unexplained. Therefore, we aimed to describe which viruses were detected in unselected patients with a suspected central nervous system infection and the first diagnostic workflow in a university hospital laboratory.
Methods:
A comprehensive virus testing in cerebrospinal fluid with an in-house real-time PCR method was employed. Determining how many and which viruses to test was at the full discretion of the treating physician.
Results:
1462 patients were evaluated from 2011 to 2017 and 9 898 viral PCRs were made: 176 subjects (12%) had a positive result. There was great heterogeneity in the frequency of patients tested for each virus, ranging from 97.9% (1431 out of 1462) for herpes simplex virus (HSV) to 1.9% (28 out of 1462) for Parvovirus B19, positive in 1 patient. Enterovirus (EV) was the leading virus detected: the frequency was higher with respect to HSV (5.2% vs 2.4%, p=0.0004), varicella-zoster virus (VZV)(5.2% vs 2.9%, p=0.0052), human herpesvirus-6 (5.2% vs 1.7%, p=0.0014) and human herpesvirus-7 (HHV-7)(5.2% vs 2.5%, p=0.0406). Both VZV (83.5%) and HSV (97.9%) were tested significantly more than EV (68.7%, p<0.0001) and HHV-7 (24.1%, p<0.0001): the latter had a positivity comparable to HSV and it was detected in younger patients (median age 29 years), as for EV (median age 35 years). There was no difference found in the age of positive subjects with respect to negative ones for the other viruses tested.
Conclusion:
EV was the fifth virus frequently included in the diagnostic workflow but the most frequently detected, mostly in subjects aged less 40, as HHV-7 was. Testing these two viruses in all younger patients could reduce the number of unknown etiology.
1. INTRODUCTION
Acute meningitis and encephalitis are Central Nervous System (CNS) diseases whose correct diagnosis is challenging because of non-specific clinical characteristics and the wide spectrum of possible etiologies, both non-infectious and infectious.The latter frequently have a viral etiology when the cause is identified. However, it is estimated that about half of patients with central nervous system infections cases remain untreated [1-3].
First-line virologic test panel for clinically suspected acute central nervous system infections in adult patients includes Polymerase Chain Reaction (PCR) for herpes simplex virus (HSV)-DNA and varicella-zoster virus (VZV)-DNA because ruling out these two herpesviruses’ positivity could allow the discontinuation of acyclovir treatment and PCR for enterovirus (EV)-RNA: EV is the leading cause of viral meningitis worldwide, and in case of confirmed EV etiology, unnecessary antibiotic treatment is avoided and hospitalization duration is reduced [4, 5]. Molecular testing of cerebrospinal fluid for HSV infection is extremely sensitive and specific (approaching to 100% for both) [6] and this diagnostic approach is sensitive, also for the detection of VZV (sensitivity and specificity values about 80% and 98%, respectively) [7] but it is slightly less reliable to identify EV because the viral load observed in the CSF is relatively low [8].
Mc Gill et al. [4], carried out a multicenter prospective observational cohort study enrolling 638 adult patients with symptoms consistent with meningitis across England from 2011 to 2014: viral etiology was identified in 38% of patients and a bacterial etiology in 16% but in 42% of subjects, no pathogen was found. The most frequent viruses detected were EV (127 patients, 20%), followed by HSV and VZV. A higher percentage of patients with no causative virus identified (46.1%) was reported by Kaminski et al. [5], in a study on aseptic infections of the central nervous system etiology including 191 adult subjects diagnosed in Germany from 2007 to 2014: the highest incidence of EV infections (36%) was found in meningitis and, conversely, HSV and VZV were the main causes of encephalitis and meningoencephalitis. Other viruses found positive with routinely PCR methods in the two studies were Epstein-Barr Virus (EBV) [4], cytomegalovirus (CMV) [4], measles virus (MEAV) [4], Mumps Virus (MUMV) [4, 5], human herpes virus-6 (HHV-6) [5] and Toscana virus [5].
Almost all published data on molecular epidemiology of suspected central nervous system infections in adult patients reported the frequency of positive detection in cerebrospinal fluid (CSF) for each specific virus and included the testing of the most important causes of neurological disease. Viruses as human herpesvirus-7 (HHV-7), which may cause CNS disease both in case of primary infection [9] and of reactivation [10], are rarely looked for; moreover, a few data on the influence of the diagnostic approach (how many and which viral PCRs were requested for each patient) in clinical practice are available.
The aim of this retrospective study was to give an integrated report of the detection of a wide spectrum of viruses such as EV, parvovirus B19 (PvB19), EBV, VZV, HHV-7, HSV, JC virus (JCV), HHV-6,MEAV, human adenovirus (HAdV), CMV, West Nile Virus (WNV), human parechoviruses (HPeVs), Tick-Borne Encephalitis Virus (TBEV), human herpesvirus-8 (HHV-8),MUMV, and human T-cell leukaemia virus type 1 (HTLV-1) identified through molecular techniques and to show the diagnostic workflow in an unselected cohort of adult patients with a clinically suspected central nervous system infection.
2. MATERIALS AND METHODS
2.1. Study Design
This is a retrospective study to investigate the prevalence of detection of viruses included in the CSF analysis requests of adult patients (age 18-64 years) with a suspected CNS acute infection. All samples selected for EV and/or HSV testing, sent to the Microbiology and Virology Unit of the University of Padova from January, 1 2011 to October, 31 2017 from hospitals of the Veneto region, were included. The requested molecular tests were at the full discretion of the treating physician and they were included in the routine diagnostic approach to the disease. When a patient had more than one sample available, only the first one was included in the statistical analysis, regardless of the time interval between the first and the subsequent samples. All samples were tested in duplicate. Samples obtained from patients with a known diagnosis of HIV infection and/or with a positive CSF culture result for bacteria, fungi or mycobacteria were excluded from the analysis. Only viruses that were tested in at least 10% of the study population and/or with a positive result were included in the study.
2.2. Laboratory Methods
The CSF samples were stored at 4 °C and processed within 24 h of arrival. The tests were performed using the protocols currently applied at the Microbiology and Virology Unit of the Padova Hospital, as previously described [11-14]. During all DNA extractions and purifications, precautions were taken to reduce the risk of false-positive results. Sample adequacy was tested by real-time PCR amplification of the β-globin gene when DNA viruses were tested, and by real-time PCR amplification of a sequence of the RNase P gene in cases of RNA viruses. EBV-DNA and CMV-DNA viral loads were expressed in copies/mL with a threshold level of 1000 copies/mL. HSV typing was performed in positive samples, as previously reported [15].
2.3. Statistical Analysis
Data collected included the subject's age (evaluated as a continuous variable and as a binary variable: 18-39 years vs 40-64 years), the number of PCRs requested (continuous variable) and the result of the molecular tests (as a categorical variable and as quantitative data for EBV-DNA and CMV-DNA). The continuous data were presented as the median and interquartile range. The Mann-Whitney U test was used to test the significance of the difference of the median between the groups of patients, while the Chi-squared test and Fisher’s exact test were used to compare categorical variables as appropriate (according to the frequencies). All statistical analyses were performed with MedCalc Statistical Software version 19.0.3 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2019).
3. RESULTS
3.1. Virus Tested and Virus Detected
The patients who had CSF tested during the study period were 1462 (764 males and 698 females): overall, 9 898 viral PCRs were made and 191 PCRs (1.9% of all PCRs) had a positive result and EV was the more frequently isolated, followed by EBV. A complete description of the relative frequency of detection of positive PCRs is reported in Fig. (1). A negligible number of tests, (n = 45, 14 patients involved) were requested but not performed because no sufficient sample was available. A total of 285 tests, all negative, were performed to detect rubella virus, Toscana virus, influenza virus, choriomeningitis virus, chikungunya virus and Zika virus: they are not discussed in the work.
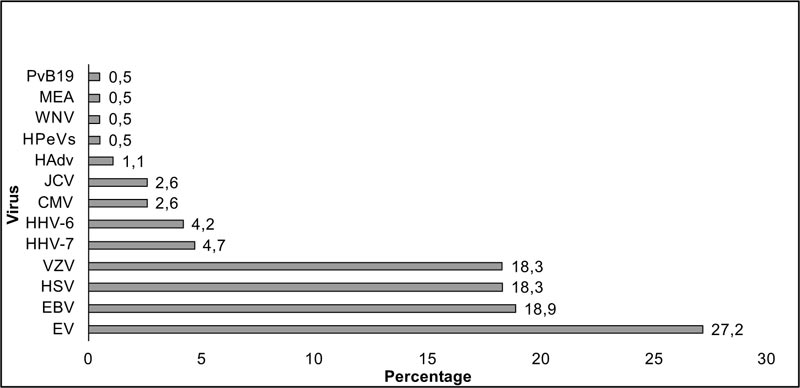
PCR: real-time polymerase chain reaction EV: enterovirus; EBV: Epstein–Barr virus; HSV: herpes simplex virus; VZV: varicella zoster virus; HHV-7: human herpes virus-7; HHV-6: human herpes virus-6; CMV: cytomegalovirus; JCV: JC virus; HAdV: human adenovirus; HPeVs: human parechoviruses; WNV: West Nile Virus; MEA: measles virus; PvB19: parvovirus B19. HHV-7 tested from January 2013. HAdV tested from February 2012. HPeVs tested from May 2012.
There was heterogeneity in the overall frequency of patients tested for each specific virus, with values ranging from 97.9% (1431 out of 1462) for HSV to 1.9% (28 out of 1462) for PvB19. A positive result was reported in 176 subjects (12%). The description of the number of patients tested, of the percentage of patients tested with respect to the 1462 patients included, the number of positive PCRs and the percentage of positive PCRs with respect to those performed for the specific virus are reported in Table 1. EV was the leading virus detected: the frequency was significantly higher respect to HSV (5.2% vs 2.4%, p = 0.0004), VZV (5.2% vs 2.9%, p = 0.0052), HHV-6 (5.2% vs 1.7%, p = 0.0014), HHV-7 (5.2% vs 2.5%, p = 0.0406) and JCV (5.2% vs 1.8%, p = 0.0139). VZV and HSV were identified in 2.9% (35 out of 1221) and in 2.4% (35 out of 1431) of samples, respectively: however, these two herpesviruses were included in the diagnostic workflow of a higher number of patients with respect to those tested for EV (68.7%, p < 0.0001). HHV-7 was tested in a small percentage of samples (353 out of 1462, 24.1%), lower than that of HSV (97.9%, 1431 out of 1462), VZV (83.5%, 1221 out of 1462), EBV (71%, 1038 out 1462) and EV (68.7%, 1005 out of 1462) (p < 0.0001) but the frequency of detection (2.5%, 9 out of 353) was comparable to that of HSV (2.4%, 35 out of 1431, but tested in 97.9% of subjects). The detection of PvB19 was confirmed in a second CSF sample tested 22 days later.
| - |
Patients Tested (n) |
Percentage of patients tested respect to the 1462 patients included | Positive PCRs (n) | Percentage of positive PCRs respect to the PCRs performed for the specific virus |
|---|---|---|---|---|
| EV | 1005 | 68.7 | 52 | 5.2 |
| PvB19 | 28 | 1.9 | 1 | 3.6 |
| EBV | 1038 | 71 | 36 | 3.5 |
| VZV | 1221 | 83.5 | 35 | 2.9 |
| HHV-7a | 353 | 24.1 | 9 | 2.5 |
| HSV | 1431 | 97.9 | 35 | 2.4 |
| JCV | 283 | 19.4 | 5 | 1.8 |
| HHV-6 | 477 | 32.6 | 8 | 1.7 |
| MEAV | 159 | 10.9 | 1 | 0.6 |
| HAdVb | 377 | 25.8 | 2 | 0.5 |
| CMV | 1078 | 73.7 | 5 | 0.5 |
| WNV | 542 | 37.1 | 1 | 0.2 |
| HPeVsc | 819 | 56 | 1 | 0.1 |
| TBEV | 443 | 30.3 | 0 | 0 |
| HHV-8 | 349 | 23.9 | 0 | 0 |
| MUMV | 148 | 10.1 | 0 | 0 |
| HTLV-1 | 147 | 10.1 | 0 | 0 |
All CMV-DNA values and 32 out of 36 EBV-DNA values were below 1000 copies/mL: the other EBV-DNA values were 1813 copies/mL, 2040 copies/mL, 38 583 copies/mL and 790 000 copies/mL.
Twenty-three HSV positive samples were HSV-1 (65.7% of HSV-DNA positive samples), 5 samples were HSV-2 (14.3%) and 7 (20%) CSFs were not typed due to the low viral load.
Almost all patients (161 of 176) reported the detection of a single viral agent: two positive PCRs were identified in 15 subjects (8.5% of positive patients). The more frequently involved was EBV (6 patients: 3 EBV-HSV, 2 EBV-VZV, 1 EBV-JCV). A complete description is reported in Table 2. The samples of patients admitted to the Padova Hospital were 532 (36.4% of all samples) and negative CSF culture was found in 256 (48.1%) out of 532 samples. The choice of not including the culture in the diagnostic workflow was at full discretion of the treating doctor, who may have decided not to perform on the basis of CSF findings. Twenty-eight patients (M/F 20/8, median age 52 years) were excluded from the study because of positive culture. We applied a strict criteria and also the 7 samples with a diagnosis of contaminating bacteria were excluded: one of these 7 samples was found positive for HSV. The viruses detected in the other 21 patients were HSV (1 patients) and EBV (2 patients). Overall, the more frequent non contaminating isolates belonged to the Staphylococcus spp. A complete description is reported in Table 3.
| Pt | Gender | Age (years) |
Total PCRs (n) | EV | PvB19 | EBV | VZV | HHV-7a | HSV | JCV | HHV-6 | MEAV | HAdVb | CMV | WNV | HPeVsc | TBEV | HHV-8 | MUMV | HTLV-1 |
| 1 | M | 20 | 7 | NEG | NEG | POS | NEG | POS | NEG | NEG | ||||||||||
| 2 | M | 24 | 10 | NEG | POS | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | |||||||
| 3 | F | 26 | 15 | NEG | NEG | POS | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | ||
| 4 | M | 27 | 4 | POS | NEG | POS (d) |
NEG | |||||||||||||
| 5 | F | 28 | 11 | POS | NEG | NEG | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | ||||||
| 6 | F | 36 | 14 | POS | NEG | NEG | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | NEG | |||
| 7 | F | 40 | 12 | NEG | NEG | POS | NEG | NEG | POS | NEG | NEG | NEG | NEG | NEG | NEG | |||||
| 8 | F | 46 | 3 | NEG | POS | POS (e) |
||||||||||||||
| 9 | F | 50 | 16 | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | |
| 10 | F | 51 | 11 | POS | NEG | NEG | NEG | NEG | NEG | NEG | NEG | POS | NEG | NEG | ||||||
| 11 | M | 53 | 6 | NEG | POS | NEG | NEG | POS | NEG | |||||||||||
| 12 | F | 54 | 6 | NEG | POS | NEG | POS (e) |
NEG | NEG | |||||||||||
| 13 | M | 55 | 6 | POS | NEG | POS (e) |
NEG | NEG | NEG | |||||||||||
| 14 | M | 61 | 10 | NEG | NEG | POS | NEG | POS | NEG | NEG | NEG | NEG | NEG | |||||||
| 15 | M | 64 | 6 | NEG | POS | POS | NEG | NEG | NEG |
EV: enterovirus; PvB19: parvovirus B19; EBV: Epstein-Barr virus; VZV: varicella zoster virus; HHV-7: human herpes virus-7; HSV: herpes simplex virus; JCV: JC virus; HHV-6: human herpes virus-6; MEAV: measles virus; HAdV: human adenovirus; CMV: cytomegalovirus; WNV: West Nile Virus; HPeVs: human parechoviruses; TBEV: tick-borne encephalitis virus; HHV-8: human herpes virus-8; MUMV: mumps virus; HTLV-1: human T-cell leukemia virus type 1.
PCR: real-time polymerase chain reaction.
aHHV-7 tested from January 2013; bHAdV tested from February 2012; cHPeVs tested from May 2012.
| - | Gender | Age | Isolates | Tested viruses | Positive viral PCRs |
|---|---|---|---|---|---|
| Pt 1 | M | 44 | Staphylococcus capitis | HSV | none |
| Pt 2 | M | 37 | Staphylococcus hominis | HSV, VZV, EV, EBV, CMV, JCV | none |
| Pt 3 | M | 41 | Pseudomonas putida | HSV, VZV, EV, EBV, CMV, HHV-6, HHV-7, HHV-8, JCV, HAdV, WNV, MUMV, HTLV-1 | none |
| Pt4 | M | 61 | Pseudomonas aeruginosa | HSV, VZV, EV, EBV, CMV, HHV-6, HHV-7, HHV-8, JCV, TBEV, HAdV, MEAV, WNV, MUMV, HTLV-1 | none |
| Pt 5 | M | 49 | Haemophilus influenzae | HSV, VZV, EV, HAdV | none |
| Pt 6 | M | 53 | Bacillus licheniformis | HSV, VZV, CMV | none |
| Pt 7 | M | 27 | Staphylococcus aureus | HSV, EV, HPeVs, EBV, CMV, HHV-6, TBEV | EBV |
| Pt 8 | F | 50 | Streptococcus agalactiae | HSV, VZV, EV, HPeVs, HAdV, MEAV | none |
| Pt 9 | M | 30 | Streptococcus agalactiae | HSV | none |
| Pt 10 | F | 60 | Staphylococcus epidermidis | HSV, EBV, CMV | none |
| Pt 11 | F | 23 | Staphylococcus haemolyticus | HSV, VZV | none |
| Pt 12 | F | 44 | Staphylococcus hominis | HSV, VZV, EV, HPeVs, EBV, CMV, HHV-6, HHV-7, HHV-8, JCV, TBEV, HAdV, MEAV, WNV, MUMV | none |
| Pt 13 | M | 59 | Mycobacterium tuberculosis – complex | HSV, EV, HPeVs, EBV, CMV, WNV | none |
| Pt 14 | M | 32 | Staphylococcus aureus | HSV, VZV, EV, HPeVs, HHV-6, HHV-7, HHV-8, JCV, TBEV | none |
| Pt 15 | M | 58 | Staphylococcus haemolyticus | HSV, EV, HPeVs, EBV, CMV | none |
| Pt 16 | M | 60 | Listeria monocytogenes | HSV, EV | none |
| Pt 17 | M | 64 | Staphylococcus hominis | HSV, VZV, EBV, CMV, HHV-8, JCV | none |
| Pt 18 | M | 37 | Staphilococcus hominis, Staphilococcus epidermidis | HSV, VZV, EV, HPeVs, EBV, CMV, HHV-6, HHV-7, HHV-8, HAdV | none |
| Pt 19 | M | 60 | Staphylococcus epidermidis | HSV, VZV, EV, HPeVs, HHV-6, HHV-7, MEAV | HSV |
| Pt 20 | F | 57 | Staphylococcus epidermidis | HSV, VZV, EBV, CMV, HHV-6, HHV-7, HHV-8, HTLV-1 | none |
| Pt 21 | F | 63 | Rothia dentocariosa | HSV, VZV, EV, HPeVs, EBV, CMV | HSV |
| Pt 22 | M | 64 | Streptococcus pneumoniae | HSV, VZV | none |
| Pt 23 | F | 48 | Mycobacterium tuberculosis – complex | HSV, VZV, EV, HPeVs, EBV, CMV, HHV-6, HHV-7, HHV-8, HAdV, MEAV, MUMV, PvB19 | EBV |
| Pt 24 | M | 52 | Staphylococcus epidermidis | HSV, VZV, EV, HPeVs, HHV-6, HHV-7, HHV-8 | none |
| Pt 25 | F | 58 | Corynebacterium sp | HSV, VZV, EV, HPeVs, EBV, CMV, MEAV | none |
| Pt 26 | M | 58 | Cryptococcus neoformans | HSV, VZV, EBV, CMV, JCV | none |
| Pt 27 | M | 40 | Staphylococcus haemolyticus | HSV, VZV, EBV, CMV, TBEV, WNV | none |
| Pt 28 | M | 57 | Cryptococcus neoformans | HSV, VZV, EBV, CMV, HHV-8, JCV | none |
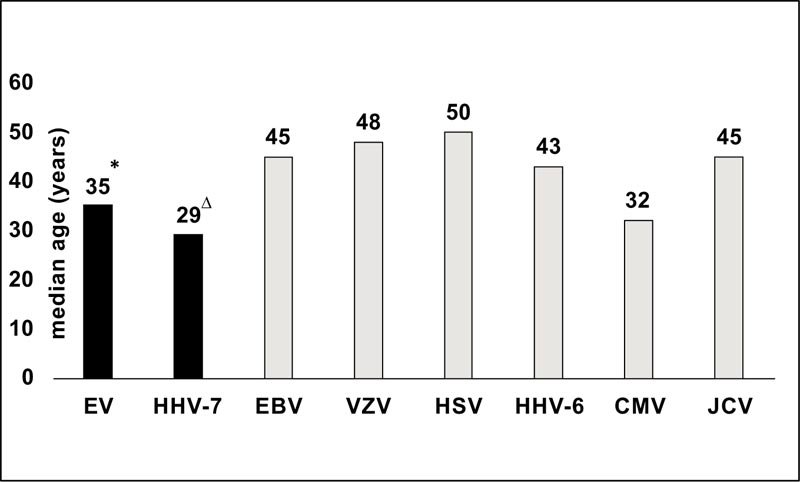
* 35 years (IQR 27 years-44 years) versus 44 years (IQR 34 years-54 years), p = 0.0001 ∆ 29 years (IQR 26 years-38 years) vs 44 years (IQR 34 years-54 years), p = 0.0285
3.2. The Role of Age
The median age of patients with a positive result was not significantly different from that of subjects with a negative result (43 years, IQR 31 years-53 years versus 45 years, IQR 34 years-54 years), but the difference in the median age between samples with the positive or negative result was significant for EV (35 years, IQR 27 years-44 years versus 44 years, IQR 34 years-54 years, p = 0.0001) and HHV-7 (29 years, IQR 26 years-38 years versus 44 years, IQR 34 years-54 years, p = 0.0285). The difference was confirmed also when the analysis focused on isolated EV positivity (p = 0.0002) and isolated HHV-7 positivity (p = 0.0307). The median age of patients evaluated and of those not evaluated was comparable both for EV testing (44 years, IQR 33 years-54 years versus 46 years, IQR 34 years-55 years) and HHV-7 testing (44 years, IQR 33 years-54 years versus 44 years, IQR 34 years-54 years).
Patients with isolated HHV-7 detection had the lowest median age and the gap was significant compared to subjects positive for EBV (p = 0.0083), for VZV (p = 0.0141) and HSV (p = 0.0135); subjects with an isolated positive PCR for EV had a lower median age compared to samples with positive PCR for EBV (p = 0.0008), VZV (p = 0.0022) and HSV (p = 0.0011) (Fig. 2).
Patients aged <40 years old had a higher overall percentage of positivity of 14.2%, while those aged 40-64 years had a percentage of 10.8%: the difference approached the significance (p = 0.0557).
The distribution by the age of viral PCRs found positive in more than two samples is described in Fig. (3).
3.3. Number of Tests Performed
The median number of tests performed in patients who showed a viral detection was significantly higher with respect to the number of tests reported in patients with negative samples (7 tests, IQR 5-9 tests versus 6 tests, IQR 4-9 tests, p = 0.0063).
The description of the percentage of patients with a positive PCR according to the number of PCRs included in the diagnostic panel is reported in Fig. (4). The percentage of positivity was higher in the 17 patients who were tested for all viruses but PvB19 (23.5%): EV was detected in all these positive samples (in one subject associated to HAdV).

EV: enterovirus; EBV: Epstein–Barr virus; HSV: herpes simplex virus; VZV: varicella zoster virus; HHV-7: human herpes virus-7; HHV-6: human herpes virus-6; CMV: cytomegalovirus; JCV: JC virus HHV-7 tested from January 2013.

HSV and EV were included in all test panels including 2 to 16 PCRs performed, but the percentage of patients tested within each group was similar for HSV (minimum 92%, maximum 100%) while had a great variability for EV (minimum 3.4%, maximum 100%): as a consequence, the median percentage of EV-RNA inclusion was lower than that of HSV-DNA (84.4% versus 98.3%, p = 0.002)
About half of patients (n = 810, 55.4%) had CSF tested for 4-7 PCRs: HSV was tested in 793 subjects (overall median percentage of testing 97.9%) and 21 (2.6%) were found positive, VZV in 701 subjects (overall median percentage of testing 87.3%) and it was detected in 18 (2.6%) and EV in 524 individuals (overall median percentage of testing 68.7%), with 23 samples positives (4.4%). In the same cohort, HHV-7 was tested in a total of 43 subjects (overall median percentage of testing 2.5%) and the virus was identified in 2 patients, with a percentage comparable to those of EV (4.6%) but a percentage of testing being significantly lower (p = 0.0209).
Only 2 subjects were tested for HHV-7 when the number of PCRs tested ranged from 1 to 3 (on a total of 178 patients) and the result was negative; conversely 308 (65%) out of the 474 patients who had 8-16 PCRs performed were tested for HHV-7 and it was detected in 7 subjects (2.3%). A complete description of which viral PCRs were prescribed and their positive and negative result for each testing set approach (intended as the number of tests requested on the sample) is reported in Supplementary Table 1.
3.4. Patients with HHV-7 Tested
Fifty patients out of 353 subjects with HHV-7 evaluated had a positive PCR (14.2%) versus 11.4% of the patients not tested for HHV-7 and the patients’ age was comparable in the two groups (median 44 years in both). In the first subgroup, HHV-7 became the third most frequently identified virus, after EV and EBV and it was found in 18% of all positive subjects. A description of the viruses tested and the viruses detected in the 353 subjects is reported in supplementary Table 2. The percentages of positivity for EV, HHV-6 and HSV were comparable with those found in patients who were not tested for HHV-7: conversely, VZV was more frequently positive in patients in whom HHV-7 was not considered as a possible reason for the SNC infection (1.2% vs 3.4%, p = 0.0447).
Clinical data were available for five patients with HHV-7 positivity: a suspected demyelinating disorder (isolated HHV-7 detection), one with a possible cerebellitis (isolated HHV-7), a suspected diagnosis of lymphocytic meningitis (2 patients, one with associated VZV positivity and one with associated EV detection) and one patient had a visual impairment and an occipital alteration at magnetic resonance imaging (HHV-7 and EV detection).
4. DISCUSSION
This study describes the molecular epidemiology of the suspected central nervous system viral infections in a large cohort of adult patients in a setting with a tertiary level diagnostic laboratory available where the extent to which PCRs are used is based on clinician’s request. We analyzed CSF results of 1462 subjects aged 18-64 years: this number is lower with respect to the work of Kleines et al. [16], referring to an 11-year period (2 604 patients), but this latter study had no age limit for inclusion and the range was 18-97 years. The same authors reported that the prevalence of positive viral PCR detection increased with age and that patients older than 80 had the highest detection rates. Moreover, Kleines’ study focused on HSV, VZV, EBV, CMV, HHV-6 and EV, while our study included a detailed analysis of the results of 17 viruses which were tested in at least 10% of the study population and/or with a positive result and reported the negative testing of other six viruses. Of note, the percentage of positive results reported in this work (4.1%) was lower than ours (12% of subjects), which is, in turn, lower than expected [17] despite the availability of many diagnostic tools: the characteristics of patients’ enrollment (no CSF alterations required) and the restriction to molecular analysis for diagnosis may explain our result. The clinical presentation of viral infections, especially encephalitis, is often non-specific and requires consideration of non-viral causes also, such as bacteria, fungi, parasites as well as non-infectious causes. However, the aim of the present study was not to describe the virologic epidemiology of confirmed viral meningitis and meningoencephalitis but to describe which viruses were detected in a suggestive clinical setting (definite diagnostic criteria could be present or not) and the first diagnostic workflow. In our study, the more frequently detected virus was EV (relative percentage 27.2%) as in the other real life retrospective studies including patients with more than one diagnosis: EV positivity relative percentage was 33.3% in the work by Calleri et al. [18], including viral meningitis and meningoencephalitis and EV positivity relative percentage was 46.6% in the study by Kaminski et al. [5], focusing on aseptic meningitis or meningoencephalitis. The differences in the percentage of detection may be not only due to our study design but also due to the different molecular methods used and the variation in the viral load of the different EV genotypes [19]. Besides EV, HSV and VZV PCRs are included in the usual initial approach to diagnosis in suspected CNS viral infections [20, 21]: overall, our relative percentage of HSV detection was slightly lower than that reported in the studies by Calleri et al. [18], and Kaminsky et al. [5], (18.4% versus 27.5% and 26.2% respectively) and the relative percentage of VZV positivity was comparable (18.4% versus 17.4% and 20.4% respectively). In our cohort. EBV-DNA detection had a higher relative positivity than HSV and VZV; this herpesvirus testing was not included in the study by Calleri and colleagues [18] while no detection was reported by Kaminski et al. [5]. This different result may be explained by the less number of tests (113 versus 1038) and by the EBV viral load we detected: 88.9% were positive at the lower limit of detection.
Surprisingly, HHV-7 was identified in an absolute percentage of patients (2.5%) higher than that of HSV even if it was requested in a significantly lower number of subjects. Of note, HSV was the only virus included with a comparable frequency both in diagnostic workflow including or excluding HHV-7 testing and this evidence may exclude a bias due to clinician decision. Our HHV-7 positive patients had a median age of 29 years (range 26 years-38 years), significantly lower compared to patients tested and found negative: this value is in accord to the cut-off age for second-line testing in case of acute encephalitis [20] and age reported in case reports describing a central nervous system infection in adult patients (median 30 years, range 26 years-35 years) [22-28]. A delayed HHV-7 primary infection was diagnosed in the case reported by Ward et al. [22], a viral reactivation was demonstrated with serology in 3 works [23, 24, 26] and suggested in one study [28] and whether the disease was due to late primary infection or reactivation was not established in two of the studies [25, 27] as it was not in our study because no serological studies and no antibody avidity were available. More than 90% of children aged less 5 years present with HHV-7 primary infection [29] and so it is possible that almost all our patients experienced a reactivation: however, it has to be underlined that we found no HHV-7 positivity in CSF of 100 patients aged more than 65 [30], despite the age-related decline in the immune function [31].
In our study, 353 patients were tested for HHV-7, a higher number with respect to the study by Corral et al. [10], who globally detected HHV-7 DNA in 5.6% of the 251 patients tested in a Spanish Hospital from 2010 to 2014: one patient had meningitis by HSV-2, 7 patients had a diagnosis of non-infectious neurological diseases but 6 subjects had a clinically compatible CNS infection, CSF changes and no other agent was detected. In Corral’s work [10], all the patients underwent the same diagnostic workflow because a multiplex PCR kit was used. Conversely, in our study, PCR selection was at the discretion of the treating doctor. HHV-7 testing was included in a set of 11 PCRs (median value), while a set of 5 PCRs (median value) was used when this herpesvirus was not chosen. The overall positivity rate of HSV, EV and HHV-6 detection (not VZV detection, more frequent in patients not tested for HHV-7) was comparable in the two sets: these data seem to suggest that there is no selection bias in the cohort of patients who were tested for HHV-7 and those who did not. We are aware that increasing the number of PCRs could give more opportunities to identify the etiology of a suspected CNS infection and that fully automated multiplex PCRs are now available [32, 33]. However we observed that the median number of tests in patients with a positive result was 7 and it was 6 in undiagnosed subjects, so the choice of the tests to include has a role as well. PvB19 was tested in 1.9% of subjects: nevertheless, we observed one positive result. Limited data on the real epidemiological scenario of CNS infection were available, but PvB19 was associated with cases of CNS infection in adult patients [34, 35] and could be included in the testing panel also as second-line testing.
In addition, age can be a simple criterion to address clinicians’ decisions. We observed that EV and HHV-7 positive patients were significantly younger than negative ones: the inclusion of these two viruses testing in the diagnostic panel of all subjects aged less than 40 could reduce the number of unknown etiologies.
Strengths of the study are the high number of patients enrolled, inclusion limited to adult subjects, the availability of 17 viral PCRs and the descriptive approach, which included both analysis of the frequency of prescribed tests and their positivity. Furthermore, the same molecular methods were applied to all samples and so data obtained throughout the study period (more than 6 years) were comparable.
Our study had two main limitations. First, it is a retrospective study and second, most clinical characteristics of the subjects enrolled and data of CSF examinations were not available, consequently, we could not perform more extensive analysis. However, we analyzed patients who underwent lumbar puncture and CSF PCR for a clinical need and routine chemistry and cellular analyses of CSF assist in CNS infection diagnosis, but microbiology tests are required to identify the etiology: patients were included in the study if they had HSV-DNA and/or EV-RNA tested and it should be pointed out that HSV-DNA may be detected in CSF specimens with normal white blood cells and protein levels [36] and that about 15% of CSF positive for EV-RNA had normal CSF cell counts [37].
CONCLUSION
In conclusion, here results are reported of a large analysis of the diagnostic approach of suspected central nervous system infections in adult patients. EV is the fourth fifth virus more frequently included in the diagnostic workflow but the most frequently detected, mostly in subjects aged less 40, was HHV-7 . The testing of these two viruses in all younger patients could reduce the number of suspected CNS infections with unknown etiology and HHV-7 serology could help in defining the clinical role of this virus.
LIST OF ABBREVIATIONS
| CMV | = Cytomegalovirus |
| CNS | = Central Nervous System |
| CSF | = Cerebrospinal Fluid |
| EBV | = Epstein-Barr virus |
| EV | = Enterovirus |
| HAdV | = Human Adenovirus |
| HHV-6 | = Human Herpes Virus-6 |
| HHV-8 | = Human Herpesvirus-8 |
| HPeVs | = Human Parechoviruses |
| HSV | = Herpes Simplex Virus |
| HTLV-1 | = Human T-Cell Leukaemia Virus Type 1 |
| JCV | = JC Virus |
| MEAV | = Measles Virus |
| MUMV | = Mumps Virus |
| PCR | = Polymerase Chain Reaction |
| PvB19 | = Parvovirus B19 |
| TBEV | = Tick-Borne Encephalitis Virus |
| VZV | = Varicella Zoster Virus |
| WNV | = West Nile virus |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study has been approved by Ethical Committee for Clinical Experimentation University of Padova, Italy, with reference number 50443/15.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures were followed in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all participants.
AVAILABILITY OF DATA AND MATERIALS
Data supporting the findings of this research are available within the article.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest regarding the publication of this article.
ACKNOWLEDGEMENTS
Declared None.
SUPPLEMENTARY MATERIAL
Supplementary material is available on the publisher's website along with the published article.

