All published articles of this journal are available on ScienceDirect.

Comparison of Dot ELISA Using GroEL Recombinant Protein as an Antigen and an Indirect Hemagglutination Assay for Serodiagnosis of Melioidosis
Authors Info & Affiliations
Abstract
Background:
Melioidosis is a disease caused by the Burkholderia pseudomallei bacterium. The mortality rate of infected patients is quite high because the symptoms are similar to those of various diseases, making it difficult to diagnose clinically and preventing the immediate treatment with effective antibiotics that is required for the management of acute infections. To provide appropriate treatment, accurate and rapid diagnosis is required.
Objective:
The aims of this study were to develop Dot ELISA using purified GroEL B. pseudomallei recombinant protein as an antigen and to compare the newly developed assay with an indirect hemagglutination assay (IHA) for the diagnosis of melioidosis.
Methods:
The GroEL recombinant protein was purified by immobilized metal affinity chromatography before being used as an antigen. The optimal conditions of the Dot ELISA were determined and used for subsequent experiments. A total of 291 serum samples were evaluated by the established Dot ELISA and IHA, using the bacterial culture method as the gold standard of melioidosis diagnosis.
Results:
The results from Dot ELISA and IHA revealed sensitivity, specificity, and accuracy of 85.7% (Dot ELISA)/64.3% (IHA), 94.4%/85.5%, and 93.1%/82.5%, respectively.
Conclusion:
These results indicate that the Dot ELISA developed is an efficient, simple, rapid and cost-effective technique for the early diagnosis of melioidosis and can be used in a local laboratory without specialized equipment.
1. INTRODUCTION
Melioidosis is a severe disease caused by the gram-negative bacillus Burkholderia pseudomallei, which can be transmitted via aerosol and causes a fatal infection affecting both humans and animals [1]. It is commonly found in soil and water in tropical and subtropical regions [1]. The main route of B. pseudomallei entry is through skin scratches, but it can also be transmitted via ingestion of contaminated water or inhalation [1-3]. Melioidosis is the third-leading cause of death from infectious diseases in Thailand after HIV and tuberculosis [4]. Many groups at high risk of B. pseudomallei infection have been reported, including patients with HIV infection, tuberculosis, thalassemia, cancer, diabetes, and renal disease [1, 5, 6].
The global prevalence of B. pseudomallei has been estimated to be 165,000 human melioidosis cases per year, mainly in Asia and Northern Australia, causing an estimated 89,000 deaths per year worldwide [7]. In northeast Thailand, it is estimated that there are 2,000 culture-confirmed melioidosis cases annually, with a fatality rate of 40% [8].
The clinical manifestations of melioidosis are varied and similar to those of other infections, ranging from subclinical infection and localized infections to acute fatal pneumonia and septicemia [5, 9]. B. pseudomallei is regularly resistant to multiple antibiotics, and a long course of antibiotics is required to prevent relapse of melioidosis. In addition, currently, there is no approved vaccine for the prevention of melioidosis [10, 11]. Accordingly, early and accurate diagnosis is imperative because treatment with specific, effective antibiotics is required.
The gold standard for the diagnosis of melioidosis is the conventional culture method from clinical specimens [12]. However, this assay often requires 2 to 7 days and has a low sensitivity (60%) [13]. In addition, there are no laboratory facilities available in endemic hospitals of Thailand, and much less specially trained microbiologists. Therefore, the local hospitals require rapid, affordable, and highly accurate diagnostic tests.
Routine serological tests are an alternative strategy for the rapid diagnosis of melioidosis. Antibody- and antigen-based methods to diagnose melioidosis have been developed. For example, the serological test indirect hemagglutination assay (IHA) is used worldwide because it is a simple and inexpensive method. However, many studies have shown that the sensitivity and specificity of this test are quite low in regions of endemicity due to the high seropositive background of healthy individuals in these reasons [14-18]. In addition, enzyme-linked immunosorbent assay (ELISA)-based methods, which are sensitive, specific, rapid, and cost-effective, have been developed [19-24].
We previously reported a good efficiency of a microtiter plate ELISA-based method to diagnose melioidosis, using recombinant GroEL (rGroEL) as an antigen [20]. However, this method is time-consuming and requires special equipment, a limitation preventing its use in local routine laboratories in Thailand. Therefore, a rapid and simple method should be developed. The objective of this study was to develop the Dot ELISA using rGroEL as antigen for the simple and rapid diagnosis of melioidosis. Moreover, the efficiency of the Dot ELISA developed was compared to that of IHA in the diagnosis of melioidosis in Thai patients, using bacterial culture as the gold standard to which these assays were compared.
2. MATERIALS AND METHODS
2.1. Human Serum Samples
This study was conducted using sera collected from 2015 to 2017. A total of 291 serum samples from Thailand were tested to evaluate the effectiveness of Dot ELISA using rGroEL proteins as an antigen and IHA for the diagnosis of melioidosis. These samples included two groups: Melioidosis patient (P) serum samples that were bacterial culture-confirmed in northeast Thailand (n=42) and a negative control group (n=249) consisting of samples from patients with other bacterial infections (OBI; n=74) and normal (N) serum samples that were collected from healthy blood donors (n=175). The OBI group consisted of serum samples from patients infected with the following bacteria: Escherichia coli (n=7), Klebsiella pneumoniae (n=19), Pseudomonas spp. (n=19), other glucose-non fermentative (GNF) bacteria (n=15), and gram-positive cocci (n=14).
2.2. GroEL Recombinant Antigen Production
Recombinant protein production was performed according to the protocol described in a previous report [20]. In brief, expression of rGroEL from a plasmid was induced by 1mM isopropyl β-D-1-thiogalactoside (IPTG; Thermo Fisher Scientific) and rGroEL protein was then purified by immobilized metal affinity chromatography (IMAC) using TALON® Metal Affinity Resin (Clontech Laboratories, Mountain View, CA, USA). The purified recombinant proteins were verified using SDS-PAGE on 12% polyacrylamide gels and stained with Coomassie Blue R-250. The concentration of purified rGroEL protein was determined by Bradford assay using bovine serum albumin (BSA; Sigma-Aldrich) as the standard. The purified rGroEL protein was stored at −80 °C until use in later assays.
2.3. Optimization of Dot ELISA Using rGroEL Protein as an Antigen
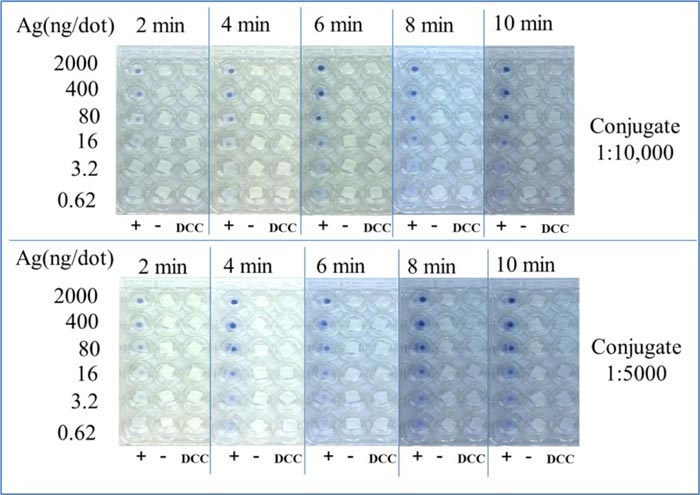
The Dot ELISA was optimized using purified rGroEL antigen for the detection of antibodies in the pooled sera from patients with B. pseudomallei infections (10 culture-positive melioidosis sera) and in control sera (10 normal sera). The assay was performed using various concentrations of coating antigen, dilutions of anti-human IgG HRP-conjugate, and incubation times with the substrate. The validation of purified rGroEL protein antigen was performed using a range of amounts of rGroEL (2000, 400, 80, 16, 3.2, and 0.62 ng/dot). A serum dilution of 1:200 was tested using the pooled positive serum samples and pooled negative serum samples. The anti-human IgG HRP-conjugate dilutions tested were 1:5000 and 1:10,000, and stop reaction times of 2, 4, 6, 8, and 10 min were tested. The optimal conditions were determined based on the conditions that showed the greatest difference between the blue dot in wells with pooled positive sera and no dot in wells with pooled negative sera, with a clear background. The established conditions were then used to investigate the serum samples.
2.4. Evaluation of the rGroEL Dot ELISA for the Diagnosis of Melioidosis
The purified rGroEL protein at optimal concentration, determined in the previous step, was dissolved in coating buffer (0.05 M carbonate buffer, pH 9.6) and then applied on a nitrocellulose membrane (50 μl) using a dot blot apparatus (Bio-Dot Microfiltration Apparatus). After the membranes were air-dried for 30 min at room temperature, each dot on the nitrocellulose membrane was cut and placed into 24-well microplates. Each dot was then blocked with 300 μl of blocking solution (2% BSA in 0.15 M phosphate-buffered saline [PBS]) at room temperature for 1 h, followed by washing with 0.05% PBS-Tween three times. Next, 300 μl of diluted serum (0.5% BSA in PBST) was added and incubated at room temperature for 30 min. After washing, 300 μl goat anti-human IgG-HRP antibody at the optimal dilution was dispensed into each well and the microplate was incubated for 30 min at room temperature. The enzymatic reaction was visualized by adding 3, 3', 5, 5'-tetramethyl benzidine (TMB) membrane substrate (KPL, Gaithersburg, MD, USA) and washed with tap water to stop the reaction at the optimal time. The direct conjugate control (DCC) was 0.5% BSA in PBST. The two-fold serial dilutions of sera tested were 1:800, 1:1600, 1:3200, 1:6400, and 1:12800, and the endpoint antibody titer was read as the last serum dilution that showed a positive result.
2.5. Indirect Hemagglutination Assay for the Diagnosis of Melioidosis
The standard IHA was performed using a commercial kit (National Institute of Health, Thailand) according to the manufacturer’s instructions. Briefly, serum samples were heat-inactivated at 56oC for 30 min, and then incubated with uncoated cells at room temperature for 30 min. The samples were centrifuged to separate the supernatants (absorbed serum), which were then diluted 1:10 before the next step. Samples were then titrated into a 96-microwell plate and melioidosis test cells were added. The final serial two-fold dilution ranged from 1:20 up to 1:1280. The reaction was allowed to proceed at room temperature for 2 h. The cell control, positive control, and negative control were used for the quality control. The presence of antibodies was established by red cell agglutination. A titer of ≥1:160 was considered positive.
2.6. Statistical Analysis
Statistical analyses were performed using the statistical software package SPSS 16.0 for Windows (SPSS). The sensitivity and specificity of Dot ELISA and IHA were evaluated using bacterial culture as the gold standard for diagnosis of melioidosis. The receiver operating characteristic (ROC) curve and the areas under the receiver operator characteristic curves (AUROCC) were determined to illustrate the sensitivity versus specificity of the Dot ELISA and IHA. The Mann–Whitney test was used to determine whether there were differences in median titer between different serum groups. Spearman’s rank correlation was performed to determine the correlation coefficient for all pairs of tests. The agreement between Dot ELISA and IHA was determined by Kappa analysis. Differences were considered statistically significant if the p-value was <0.05.
3. RESULTS
3.1. Optimization of Dot ELISA
The optimal conditions of Dot ELISA were validated using a pool of 10 positive sera and a pool of 10 negative sera. The quantity of rGroEL antigen, the dilution of the conjugate, and the reaction period of the substrate were tested. The results, shown in Fig. (1), revealed that the optimal antigen concentration was 80 ng/dot, conjugate dilution was 1:5000, and reaction time with the substrate was 4 min. Under these optimized conditions, the reaction from the pooled positive serum samples provided a clear blue dot, with no color surrounding the dot, and the wells containing the DCC and the pooled negative serum samples had no color on the dot.
3.2. Evaluation of the rGroEL Dot ELISA and IHA for the Diagnosis of Melioidosis
A total of 291 serum samples were evaluated. The optimized conditions were used for the rGroEL Dot ELISA, with sera diluted in a two-fold serial dilution (1:800, 1:1600, 1:3200, 1:6400, and 1:12800). The cut-off titer value of Dot ELISA was investigated at ≥1:800, ≥1:1600, and ≥1:3200, as shown in Table 1. The suitable cut-off titer value was ≥1:1600, which provided the highest accuracy (93.1%) with good sensitivity (85.7%), specificity (94.4%), positive predictive value (72.0%), and negative predictive value (97.5%). The IHA was also performed using a cut-off titer value of ≥1:160, according to the manufacturer’s recommendation. The IHA exhibited sensitivity, specificity, positive predictive value, negative predictive value, and an accuracy of 64.3%, 85.5%, 42.9%, 93.4%, and 82.5%, respectively (Table 1).
3.3. Comparison Between the Dot ELISA and IHA for the Diagnosis of Melioidosis
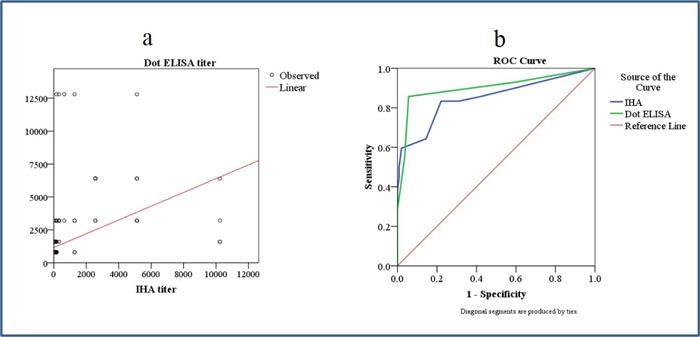
The 291 serum samples were verified by Dot ELISA, and the end-point titer was calculated. The results revealed that the geometric mean (GM) of the Dot ELISA titer of the P group (2,804.0) was higher than that of the OBI (928.9) and N (822.1) groups. The individual B. pseudomallei antibody titers, presented in a box plot in Fig. (2a), showed a significant difference between the median titers of each group (p<0.001). The GM titers from the IHA assay are shown in a box plot of individual titers in each serum group, as shown in Fig. (2b). There was a significant difference in median titer between the P (472.1) and OBI (46.8) groups and between the P (472.1) and N (27.0) groups (p<0.001), but not between the N (27.0) and OBI (46.8) groups (p=0.448).
| Cut-off titer | Melioidosis Serum (n=42) | Non-Melioidosis Serum (n=249) | Percentage | ||||||
|---|---|---|---|---|---|---|---|---|---|
| + | - | + | - | SE | SP | PPV | NPV | ACC | |
| Dot ELISA | 39 | 3 | 147 | 102 | 92.9 | 41 | 21 | 97.1 | 48.5 |
| ≥1:800 | |||||||||
| Dot ELISA | 36 | 6 | 14 | 235 | 85.7 | 94.4 | 72 | 97.5 | 93.1 |
| ≥1:1600 | |||||||||
| Dot ELISA | 23 | 19 | 9 | 240 | 54.8 | 96.4 | 71.9 | 92.7 | 90.4 |
| ≥1:3200 | |||||||||
| IHA | 27 | 15 | 36 | 213 | 64.3 | 85.5 | 42.9 | 93.4 | 82.5 |
| ≥1:160 | |||||||||
The correlation between the results from the Dot ELISA and IHA was evaluated Fig. (3a), revealing a correlation coefficient of 0.482 (p=0.01). To compare the efficacy of Dot ELISA and IHA, we also analyzed the ROC curves. The AUROCC from the Dot ELISA results was higher than that of IHA (0.901 vs. 0.849, respectively; Fig. (3b). Moreover, there was a medium-level agreement between the Dot ELISA and IHA (kappa=0.59; (Table 2). The concordance and discordance of the diagnostic results between the Dot ELISA and IHA are shown in Table 2.

| Method | IHA (n) | Total | Kappa Value | P-value | ||
|---|---|---|---|---|---|---|
| + | - | |||||
| Dot ELISA (n) | + | 38 | 12 | 50 | 0.595 | 0.000 |
| - | 25 | 216 | 24 | |||
| Total | 63 | 228 | 291 | |||
In addition, the results demonstrated more false-positive samples in the OBI group by IHA (27.0%) than by the Dot ELISA (12.2%; (Table 3). The false-positive results of IHA were found in all types of OBI except gram-positive cocci and were most commonly found in the other GNF group (40%). In contrast, the false-positive results from the Dot ELISA were found in K. pneumonia, Pseudomonas spp., and other GNF bacteria and were most prevalent in other Pseudomonas spp. (44.4%).
| OBI (n) | IHA | Dot ELISA | ||
|---|---|---|---|---|
| Positive | Positive | |||
| n | % | n | % | |
| Escherichia coli (7) | 3 | 15 | 0 | 0 |
| Klebsiella pneumoniae (19) | 6 | 30 | 3 | 33.3 |
| Pseudomonas spp. (19) | 3 | 15 | 4 | 44.4 |
| Other GNF bacteria (15) | 8 | 40 | 2 | 22.2 |
| Gram-positive cocci (14) | 0 | 0 | 0 | 0 |
| Total (74) | 20 | 100 | 9 | 100 |
Moreover, we found 16 false-positive samples in the N group out of 175 samples verified by IHA. More false-positive samples were collected from the endemic area (n=11) than from the non-endemic area (n=5). Whereas the Dot ELISA found false-positive samples from the N group lower (4/175) than for IHA (16/175) and had an equal prevalence in both endemic and non-endemic areas (2/2).
4. DISCUSSION
An efficient and simple diagnostic test for melioidosis is needed to effectively manage this lethal infectious disease that is reported worldwide, as effective antimicrobial treatment could lead to reduced mortality.
IHA is a public screening test for diagnosing melioidosis. Although this assay is inexpensive and requires no special equipment, it is time-consuming. Moreover, previous studies have confirmed that IHA shows low sensitivity, low specificity, and high background antibody titers in healthy people from endemic areas [14-18].
ELISA is an attractive platform for the development of serologic tests. Previously, we developed a microtiter plate ELISA method to diagnose melioidosis based on purified rGroEL antigen that demonstrated high sensitivity (92%) and specificity (88%) [20]. In order to supply remote endemic areas with an effective, simple, and rapid serological test, this study developed Dot ELISA using purified rGroEL as antigen.
The Dot ELISA we developed relies on indirect ELISA antibody detection in serum using nitrocellulose membrane as a solid phase. The results revealed that a low antigen concentration was required (80 ng/dot), making the test less costly. Moreover, the Dot ELISA developed is rapid, with results available approximately 1 h after the blocking step, and results can be read with the naked eye. In addition, we tested a faster condition in which the amount of antigen and the concentration of the conjugated antibody were increased. Using these conditions, results were obtained within approximately 20 min (data not shown). Thus, we suggest that this is a valuable method to further develop as a rapid test and is suitable for the assessment of mass-produced kits used in a common laboratory. Moreover, Dot ELISA could be developed as a rapid point-of-care serological test.
Our study demonstrates a significant difference between the median titer of melioidosis patient and non-patient (OBI and N) sera groups by Dot ELISA. This suggests that Dot ELISA was able to discriminate between melioidosis patients and individuals without melioidosis. The cut-off titer (≥1:1600) for evaluation of the efficacy of this Dot ELISA was determined based on the titer that produced the highest accuracy. The results revealed very good sensitivity (85.7%), specificity (94.4%), and accuracy (93.1%). The results also demonstrated a high efficiency for diagnosis of melioidosis that was better or comparable to the efficiencies reported in previous ELISA studies, which presented sensitivities and specificities of 41%–90.4% and 59%–96%, respectively [19, 20, 23, 25, 26]. However, these previous studies used different antigens and tested different areas.
In this study, the results confirmed the low diagnostic sensitivity of IHA (64.3%). This is similar to the results of previous reports that demonstrated IHA sensitivities ranging from 57.3% to 69.5% [27-29]. These findings indicated that the Dot ELISA is much improved compared with the current serological method, the IHA, in terms of both sensitivity (85.7% vs. 64.3%, respectively) and specificity (94.4% vs. 85.5%, respectively). The higher AUC of the Dot ELISA (0.966) than the IHA (0.895) confirms the improved performance of the Dot ELISA.
Our data indicated that a medium-level agreement in the diagnosis results between IHA and Dot ELISA (k=0.59). The differences in results may be due to an increased specificity of purified rGroEL for melioidosis antibody compared to the crude antigen used in IHA. Moreover, in this study, the cross-reactivity of non-melioidosis antibodies within the normal group by IHA was higher than by Dot ELISA (IHA, 16 samples, Dot ELISA, 4 samples). Notably, 11 of the 16 false-positive IHA samples were collected from melioidosis endemic area. This might be due to the low sensitivity of IHA in endemic regions.
There were 20 false-positive samples in the OBI group by IHA (sera from patients infected with Escherichia coli, K. pneumoniae, Pseudomonas spp., and other GNF bacteria); meanwhile, only 9 sera revealed non-specific binding with Dot ELISA (sera from patients infected with Pseudomonas spp., K. pneumoniae, and other GNF bacteria). This result is not surprising, as the IHA uses crude antigens that may be more reactive to non-specific antibodies than the purified protein antigen (rGroEL) used in the Dot ELISA we developed. However, in our further work, we will consider using the truncated rGroEL protein to improve the Dot ELISA by reducing cross-reaction with non-melioidosis antibodies in areas with a high prevalence of melioidosis.
CONCLUSION
We report for the first time the efficiency of the Dot ELISA using rGroEL for the diagnosis of melioidosis and compare it to IHA with various serum samples by using bacterial culture as gold standard for melioidosis diagnosis. The present study demonstrates the effectiveness of the Dot ELISA as a potential method for the rapid, simple, cost-effective, and efficient serodiagnosis of melioidosis in resource-poor regions where melioidosis is endemic. Collectively, the results presented herein suggest that Dot ELISA using rGroEL antigen is an appealing candidate for further development of a rapid point-of-care test.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee of Rangsit University Thailand (approval number RSEC 01/2558).
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed in this study are included in this published article.
FUNDING
This project was funded by Rangsit University, Thailand.
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We are grateful for the support of Sunpasitthiprasong Hospital, Udon Thani Hospital, Khon Kaen Hospital, and Nakhon Phanom Hospital, Thailand. We thank Suporn Paksanont, Natnaree Saiprom, Saowaree Srisawat, Rungnapa Phunpang, and Peeraya Ekchariyawat for laboratory support and data collection. We would like to thank Phitchapat Nimnuch for the normal samples collection. We thank Jutamas Jaiyen, Benyapa Hiruntongch and Surawee Sanpanich for laboratory support.

