All published articles of this journal are available on ScienceDirect.

Antibiotic Resistance and Resistant Genes among Isolates from Diabetic Patients with Urinary Tract Infections at Benjamin Mkapa Hospital: A Cross-Sectional Study
Abstract
Introduction
The emergence of antibiotic-resistant bacteria is a growing public health concern that complicates the prevention, control, and management of bacterial infections and has become a global challenge. Urinary tract infections (UTIs), which are among the most common bacterial infections worldwide, are increasingly associated with antibiotic-resistant pathogens. The present study focused on determining both the phenotypic and genotypic characteristics of antimicrobial-resistant bacteria isolated from diabetic patients with UTIs at Benjamin Mkapa Hospital in the Dodoma region, Tanzania.
Methods
This hospital-based cross-sectional study was conducted at Benjamin Mkapa Hospital (BMH) in Dodoma, Tanzania. Midstream urine samples were collected and inoculated onto blood agar and Cystine–Lactose–Electrolyte-Deficient (CLED) agar. Antibiotic susceptibility testing (AST) was performed using the Kirby–Bauer disc diffusion method, and results were interpreted according to the 2024 Clinical and Laboratory Standards Institute (CLSI) guidelines. Data were expressed as percentages and proportions. Sequencing results were analysed using the BLAST online search tool.
Results
Out of 419 cultured samples, 261 (62.3%) showed significant bacterial growth. The isolates included coagulase-negative staphylococci (CoNS), Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Staphylococcus aureus. The majority of the isolates were susceptible to amikacin (97%), piperacillin–tazobactam (72%), imipenem (78%), and meropenem (89%). The following genes were detected among the isolates: blaCTX-M-15, blaOXA-1, blaNDM-5, blaTEM-1B, aac(3)-IId, qnrS1, aacA-aphD, blaSHV, and blaTEM.
Discussion
This study investigated antimicrobial resistance patterns and associated resistance genes among uropathogens isolated from diabetic patients with UTIs at Benjamin Mkapa Hospital, Dodoma. Out of 419 samples, 261 (62%) yielded bacterial isolates, with Escherichia coli being the most prevalent. All isolates were multidrug-resistant, showing high resistance to commonly used antibiotics such as ceftazidime, amoxicillin/clavulanic acid, ciprofloxacin, and ampicillin, but retained susceptibility to meropenem, amikacin, and imipenem. Molecular analysis revealed the presence of key resistance genes, including blaNDM-5, blaCTX-M-15, and qnrS1. These results indicate a high burden of antimicrobial resistance among diabetic patients with UTIs and emphasize the importance of integrating molecular diagnostics into routine laboratory practice.
Conclusion
Screening for antibiotic resistance genes in parallel with antibiotic susceptibility testing is important for the control and management of resistant isolates.
1. INTRODUCTION
Antimicrobial resistance has become a serious public health concern, with the transmission of resistance genes and resistant bacteria being a major focus of global attention [1]. Onanuga et al. (2020) reported that multidrug-resistant bacteria pose a significant health threat, complicating the treatment of urinary tract infections due to the limited availability of effective antibiotics. They further noted that urinary tract infections are among the most commonly diagnosed bacterial infections in hospital settings, resulting in substantial antibiotic prescribing following clinical consultations [2].
The widespread use of antibiotics for urinary tract infections (UTIs) has accelerated the emergence of antimicrobial resistance, contributing to increased morbidity, prolonged hospital stays, and higher treatment costs, thereby constituting a major public health concern [1, 2]. UTIs are particularly common among diabetic patients, affecting nearly all age groups and occurring at a much higher rate than among non-diabetic individuals [3].
Many studies have investigated antimicrobial resistance primarily through phenotypic characterisation, often overlooking the contribution of genetic determinants to resistance. Therefore, the present study aimed at determining the phenotypic and genotypic characteristics of antimicrobial-resistant bacteria extracted from diabetic patients with UTIs at Benjamin Mkapa Hospital in the Dodoma region, Tanzania.
2. METHODOLOGY
2.1. Study Design and Setting
This was a hospital-based cross-sectional study conducted from May to December 2024 at Benjamin Mkapa Hospital. Midstream urine samples were collected from diabetic patients with urinary tract infections (UTIs) for culture and sensitivity testing. Laboratory investigations were performed at the University of Dodoma Teaching Laboratory. All isolated bacteria were analyzed for identification and antimicrobial susceptibility.
2.2. Eligibility
2.3. Sample Size and Sampling Techniques
The study involved 399 individuals, as determined by the formula (1) presented below. The sample size was calculated based on the study population, defined as the annual number of patients attending the hospital across all departments (252,000).

Where;
N stands for the study population.
e stands for precision level.
95% confidence level of 0.05 was considered.
n = 399.3660856
n = 399
Twenty participants (5%) were non-respondents, resulting in a total sample size of 419. To recruit the estimated sample size, a convenience sampling technique was used.
2.4. Data and Specimen Collection
Demographic details and related factors were collected using a validated and pre-tested questionnaire. All participants were given instructions on how to collect midstream urine (MSU) for culture and susceptibility testing. The collected urine samples were sent to the laboratory for investigation and processed immediately. When immediate processing was not feasible, samples were stored at cold temperatures until culture to minimize overgrowth and preserve organism viability.
2.5. Isolation and Identification of Bacteria
After obtaining written informed consent, socio-demographic characteristics were collected using pre-tested questionnaires. Midstream urine samples were obtained from diabetic patients aged 30 years or older with urinary tract infections (UTIs) for bacterial culture and identification. The urine samples were inoculated onto CLED and blood agar plates and incubated at 37°C for 24 hours [4]. Significant bacteriuria was defined as ≥105 CFU/mL of a single bacterial species [4]. Isolated bacteria were identified based on colony morphology, Gram staining, and biochemical tests, including catalase, coagulase, sulfide indole motility (SIM), Kligler iron agar (KIA), citrate, oxidase, and urease tests.
2.5.1. Gram Staining
Gram-positive bacteria appeared purple to bluish, while Gram-negative bacteria appeared reddish to pinkish.
2.5.2. Catalase Test
A drop of hydrogen peroxide was placed on a glass slide, and bacterial colonies were introduced using an applicator stick. A positive reaction was indicated by the appearance of bubbles within 20 seconds; a negative reaction showed no bubbles.
2.5.3. Coagulase Test
Bacterial colonies were mixed with plasma on a glass slide. A positive reaction was indicated by the presence of clots, while a negative reaction was indicated by the absence of clots.
2.5.4. Sulfide Indole Motility (SIM) Test
SIM medium was inoculated by stabbing colonies and incubated at 37°C for 18–24 hours. Hydrogen sulfide production was indicated by the blackening of the media. Indole production was indicated by a red ring on top of the media after the addition of Kovac’s reagent. Motility was indicated by diffuse growth away from the stab line; non-motile organisms grew only along the stab line.
2.5.5. Kligler Iron Agar (KIA) Test
KIA was inoculated by stabbing the butt and streaking the slant, then incubated at 37°C for 18–24 hours. Acidic or alkaline reactions were determined by color changes on the slant and butt. Hydrogen sulfide production was indicated by black precipitate formation.
2.5.6. Citrate Test
The medium was inoculated by stabbing the butt and streaking the slant, then incubated at 37°C for 18–24 hours. A positive reaction was indicated by a color change from green to blue, while a negative reaction remained green.
2.6. Susceptibility Testing of Antimicrobials
A suspension of isolated microorganisms was prepared, and turbidity was adjusted to match a 0.5 McFarland turbidity standard. Antimicrobial susceptibility testing (AST) was performed using the Kirby–Bauer disk diffusion method. The inoculated Mueller–Hinton agar (MHA) plates were incubated at 37°C for 16–18 hours. The following antimicrobial agents were tested based on local treatment guidelines: amoxicillin/clavulanic acid (20/10 µg), ampicillin (10 µg), gentamicin (10 µg), ceftazidime (30 µg), piperacillin/tazobactam (100/10 µg), ceftriaxone (30 µg), ciprofloxacin (5 µg), nitrofurantoin (100 µg), cefoxitin (30 µg), amikacin (30 µg), meropenem (10 µg), and imipenem (10 µg). All antibiotic disks were obtained from Oxoid UK Ltd. Reference strains of Staphylococcus aureus (ATCC 25923), Escherichia coli (ATCC 25922), Klebsiella pneumoniae (ATCC 700603), and Pseudomonas aeruginosa (ATCC 27853) were used to validate antimicrobial susceptibility testing. Zones of inhibition were measured and reported in millimeters (mm) according to the 2024 CLSI guidelines.
2.7. DNA Extraction for Molecular Techniques
DNA extraction for molecular analysis was performed according to the protocol described by Dashti et al. (2009) using the Gentra Puregene DNA Isolation Kit. Five microliters (5 µL) of extracted DNA was mixed with 45 µL of pre-aliquoted Reddy-Load PCR Mix, containing 1.25 units of Taq DNA polymerase, 75 mM Tris-HCl (pH 8.8), 20 mM (NH4)2SO4, 1.5 mM MgCl2, 0.01% (v/v) Tween 20, 0.2 mM of each deoxynucleotide triphosphate (dATP, dCTP, dGTP, and dTTP), and picomoles of each primer. Primers for detection of antimicrobial resistance genes - version 06.11.2018 were used (Appendix 1). PCR amplification was performed in a programmable thermal cycler [5]. The reaction included an initial denaturation at 95°C for 5 minutes, followed by 32 cycles of denaturation at 94°C for 1 minute, annealing at 57°C for 1 minute, and extension at 70°C for 1 minute, with a final extension at 72°C for 10 minutes.
PCR products were purified by ethanol precipitation. Twenty-five microliters (25 µL) of template suppression reagent (TSR) was added to the pellet, mixed, and heated at 95°C for two minutes. For sequencing PCR, 1 µL of each PCR product was mixed with 3.2 picomoles of either the forward or reverse primer and 8 µL of dye-terminator-ready reaction mix. Sequencing PCR was performed in a thermal cycler programmed for 30 cycles of 96°C for 20 seconds, 50°C for 20 seconds, and 60°C for four minutes. The PCR products were purified again and stored on ice until sequencing using an automated DNA sequencer [5]. Representative agarose gel electrophoresis of PCR products from E. coli isolates carrying the various tested resistant genes is shown in Appendix 2.
2.8. Data Analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 20. Descriptive data were presented as proportions and percentages, while continuous data were summarized using the median and interquartile range (IQR). Sequencing results were analyzed using BLAST, an online sequence alignment tool.
2.9. Ethical Considerations
Ethical approval for the study (Ref. No. OUT/PG202000391) was granted by the Open University of Tanzania, and a certificate of ethical clearance (Ref. No. NIMR/HQ/R.8a/Vol.IX/4640) was obtained from the National Institute for Medical Research (NIMR), Tanzania. Participation in this study was entirely voluntary, and written informed consent was obtained from all participants before enrollment.
3. RESULTS
Midstream urine samples were collected from 419 diabetic patients diagnosed with urinary tract infections. Of these, 261 (62.3%) showed significant bacterial growth, whereas 158 (37.7%) showed non-significant growth. The majority of participants were female (219, 52%). Most participants were aged 50–59 years (160, 38%), with a median age of 58 years (IQR: 52–65). Primary school education was the most common level of education (167, 40%), and most participants were self-employed (178, 43%). Nearly half of the participants belonged to the lower-income category (207, 49%).
The bacterial isolates included Escherichia coli, coagulase-negative staphylococci (CoNS), Staphylococcus aureus, Klebsiella pneumoniae, and Pseudomonas aeruginosa. Susceptibility to amikacin, meropenem, piperacillin–tazobactam, and imipenem was 97%, 89%, 72%, and 78%, respectively. Varying degrees of resistance were observed for ampicillin (61%), ceftriaxone (39%), ceftazidime (92%), cefoxitin (41%), ciprofloxacin (64%), amoxicillin/clavulanic acid (65%), gentamicin (47%), and nitrofurantoin (64%) (Table 1).
| Antibiotics | Sensitive n (%) | Intermediate n (%) | Resistant n (%) |
|---|---|---|---|
| AM(10 µg) | 80(31) | 0(0) | 159(61) |
| FOX (30µg) | 131(50) | 0(0) | 108(41) |
| AK(30µg) | 254(97) | 0(0) | 7(3) |
| CIP(5 µg) | 87(33) | 7(3) | 167(64) |
| NIT (100 µg) | 65(25) | 28(11) | 168(64) |
| CN(10 µg) | 109(42) | 29(11) | 123(47) |
| PIT(100/10µg) | 189(72) | 29(11) | 43(17) |
| AMC (20/10µg) | 92(35) | 0(0) | 169(65) |
| CAZ(30 µg) | 7(2) | 15(6) | 239(92) |
| CRO(30 µg) | 110(42) | 50(19) | 101(39) |
| MRP(10µg) | 232(89) | 7(3) | 22(8) |
| IPM (10 µg) | 203(78) | 29(11) | 29(11) |
Abbreviations: AM, Ampicillin; FOX, Cefoxitin; CN, Gentamycin; AK, Amikacin; CIP, Ciprofloxacin; PIT, Piperacillin-Tazobactam; MRP, Meropenem; AMC, Amoxicillin/Clavulanic; CAZ, Ceftazidime; CRO, Ceftriaxone; NIT, Nitrofurantoin; IPM, Imipenem; µg, Microgram.
Out of 261 cultured samples with significant growth, Escherichia coli (109, 41.8%) was the most prevalent bacterial isolate, followed by Staphylococcus aureus (79, 30.3%), coagulase-negative staphylococci (CoNS) (36, 13.8%), Pseudomonas aeruginosa (22, 8.4%), and Klebsiella pneumoniae (15, 5.7%). Varying resistance patterns were observed among the isolates to the tested antibiotics. E. coli showed high resistance to ceftazidime (88%), amoxicillin/clavulanic acid (73%), ciprofloxacin (60%), and ampicillin (59%). CoNS exhibited 100% resistance to ampicillin, cefoxitin, amikacin, amoxicillin/clavulanic acid, and ceftazidime. S. aureus showed high resistance to ceftazidime (100%), ampicillin (91%), ciprofloxacin (82%), and nitrofurantoin (82%). K. pneumoniae was highly resistant to nitrofurantoin and gentamicin (both 100%) and ciprofloxacin (53%). P. aeruginosa exhibited high resistance to ampicillin, nitrofurantoin, and ceftazidime (all 100%), as well as ciprofloxacin (68%) (Table 2).
| Isolates | AM n(%) |
FOX n(%) |
AK n(%) |
CIP n(%) |
NIT n(%) |
CN n(%) |
PIT n(%) |
AMC n(%) |
CAZ n(%) |
CRO n(%) |
MRP n(%) |
IPM n(%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E.coli(N=109) | 65(59) | 36(33) | 0(0) | 65(60) | 44(41) | 51(47) | 36(33) | 80(73) | 95(88) | 51(47) | 15(14) | 22(20) |
| CoNS (N=36) | 36(100) | 36(100) | 36(100) | 14(39) | 22(62) | 14(39) | 0(0) | 36(100) | 36 (100) |
14(39) | 0(0) | 0(0) |
| S.aureus(N=79) | 72(91) | 36(46) | 7(9) | 65(82) | 65(82) | 36(46) | 7(9) | 36(46) | 79 (100) |
29(37) | 7(9) | 7(9) |
|
K.pneumoniae (N=15) |
7(47) | 0(0) | 0(0) | 8(53) | 15(100) | 15(100) | 0(0) | 7(47) | 7(47) | 0(0) | 0(0) | 0(0) |
|
P.aeruginosa (N=22) |
22(100) | NA | 0(0) | 15(68) | 22(100) | 7(32) | 0(0) | NA | 22 (100) |
7(32) | 0(0) | 0(0) |
Abbreviations: AM, Ampicillin; FOX, Cefoxitin; AK, Amikacin; CIP, Ciprofloxacin; CN, Gentamycin; PIT, Piperacillin-Tazobactam; AMC, Amoxicillin/Clavulanic; CAZ, Ceftazidime; MRP, Meropenem; CRO, Ceftriaxone; NIT, Nitrofurantoin, IPM, Imipenem; µg,Microgram.
The isolates exhibited multidrug resistance to the tested antibiotics, which was defined as resistance to two or more antibiotics. Among the 109 E. coli isolates, 25 (23%) were resistant to six of the tested antibiotics. Of the 79 S. aureus isolates, 28 (35%) were resistant to more than six antibiotics. Among 36 coagulase-negative staphylococci (CoNS) isolates, 21 (58%) were resistant to five antibiotics. Of the 15 K. pneumoniae isolates, 9 (60%) were resistant to three antibiotics, and among 22 P. aeruginosa isolates, 11 (50%) were resistant to three antibiotics (Table 3).
| Isolate | Resistance n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| R0 | R1 | R2 | R3 | R4 | R5 | R6 | ˃R6 | |
| E.coli (N=109) | 0(0) | 0(0) | 17(16) | 0(0) | 20(18) | 24(22) | 25(23) | 23(21) |
| S.aureus(N=79) | 0(0) | 0(0) | 0(0) | 12(15) | 24(30) | 15(19) | 0(0) | 28(35) |
| CoNS (N=36) | 0(0) | 0(0) | 0(0) | 0(0) | 0(0) | 21(58) | 9(25) | 6(17) |
| K.pneumoniae (N=15) | 0(0) | 0(0) | 0(0) | 9(60) | 6(40) | 0(0) | 0(0) | 0(0) |
| P.aeruginosa (N=22) | 0(0) | 0(0) | 0(0) | 11(50) | 0(0) | 6(27) | 5(23) | 0(0) |
Note: R0, Sensitive to all tested antibiotics; R1, R2, R3, R4, R5, R6, ˃R6, Resistant to one, two, three, four, five, six, and more than six of the tested antibiotics.
Among the 261 sequenced isolates, Escherichia coli (109, 41.8%) was the most prevalent, followed by Staphylococcus aureus (79, 30.3%), coagulase-negative staphylococci (CoNS) (36, 13.8%), Klebsiella pneumoniae (15, 5.7%), and Pseudomonas aeruginosa (22, 8.4%). Of the 109 sequenced E. coli isolates, 58 (53.2%) carried at least one resistance gene, including blaOXA-1, blaNDM-5, blaTEM-1B, and blaCTX-M-15, which are associated with resistance to carbapenems, cephalosporins, and penicillins. Additionally, 30 (27.5%) E. coli isolates harbored the aac(3)-IId gene, conferring resistance to aminoglycosides, while 15 (13.8%) carried the qnrS1 gene, associated with resistance to quinolones. Six (5.5%) E. coli isolates did not carry any resistance genes.
Among the 79 S. aureus isolates, 12 (15.2%) harbored the aacA-aphD gene, conferring resistance to aminoglycosides, whereas the remaining 67 (84.8%) isolates carried no resistance genes. Of the 15 sequenced K. pneumoniae isolates, 8 (53.3%) carried the blaSHV and blaTEM genes, which confer resistance to cephalosporins and penicillins, while the remaining 7 (46.7%) isolates had no resistance genes. No resistance genes were detected in the sequenced CoNS or P. aeruginosa isolates (Table 4).
| Isolates | Antibiotic Class | **AMR Gene | Antibiotics | Resistant Isolates n(%) |
|---|---|---|---|---|
| E.coli (N=109) | Aminoglycoside | aac(3)-IId | Gentamicin | 51(47) |
| Beta -Lactam |
blaCTX-M-15 blaNDM-5,blaOXA-1, and blaTEM-1B |
Ceftazidime Ceftriaxone Cefoxitin Meropenem Imipenem Amoxicillin/clavulanic acid Ampicillin |
95(88) 51(47) 36(33) 15(14) 22(20) 80(73) 65(59) |
|
| Quinolone | qnrS1 | Ciprofloxacin | 65(60) | |
| S.aureus (N=79) | Aminoglycoside | aacA-aphD | Gentamicin | 36(46) |
|
K. pneumoniae (N=15) |
Cephalosporins, Penicillin | blaSHV, blaTEM | Ceftazidime Ampicillin |
7(47) 7(47) |
Note: **AMR gene, Antimicrobial resistance gene
The nucleotide sequences generated in this study have been deposited in GenBank under accession numbers PZ398285, PZ404306 and PZ407646-PZ407652.
4. DISCUSSION
This study aimed to determine antimicrobial resistance patterns and associated resistance genes among isolates from patients with diabetes mellitus (DM) suffering from urinary tract infections (UTIs). A total of 261 (62%) isolates from 419 cultured samples were analyzed.
The bacterial isolates included E. coli (109, 26%), S. aureus (79, 19%), coagulase-negative staphylococci (CoNS) (36, 9%), K. pneumoniae (15, 4%), and P. aeruginosa (22, 5%). E. coli was the most frequently isolated organism, consistent with previous studies from Eastern India, Dhaka, Bangladesh, Dilla University, Ethiopia, and Ghana [3, 6–9]. The high prevalence of E. coli may be attributed to its commensal presence in the bowel, fecal contamination, and strong adhesion to epithelial cells in diabetic individuals [6, 8].
All 261 isolates (100%) exhibited multidrug resistance (MDR), defined as resistance to two or more antibiotics. This rate was higher than reported in studies from India and Ethiopia [6, 8], and may reflect poor adherence to antibiotic regimens, misuse of antibiotics, and over-the-counter availability. High resistance rates were observed for ceftazidime (92%), amoxicillin/clavulanic acid (65%), nitrofurantoin (64%), ciprofloxacin (64%), and ampicillin (61%). Conversely, isolates were highly susceptible to meropenem (89%), amikacin (97%), imipenem (78%), and piperacillin–tazobactam (72%) [10, 11]. Differences in resistance across studies may be influenced by geographic location, antibiotic availability, and prescribing practices.
E. coli isolates demonstrated high resistance to ceftazidime (88%), amoxicillin/clavulanic acid (73%), ciprofloxacin (60%), and ampicillin (59%), slightly higher than reports from Dhaka, , Surabaya, Indonesia, and Saudi Arabia [7, 12, 13], but lower than Addis Ababa, Ethiopia [14]. CoNS exhibited 100% resistance to ampicillin, cefoxitin, amikacin, amoxicillin/clavulanic acid, and ceftazidime, consistent with findings from Ethiopia [8]. S. aureus isolates were 91% resistant to ampicillin, 82% resistant to ciprofloxacin and nitrofurantoin, and 100% resistant to ceftazidime, exceeding resistance rates reported in Surabaya, Indonesia [12]. K. pneumoniae isolates were 100% resistant to nitrofurantoin and gentamicin, and 53% resistant to ciprofloxacin, showing higher or comparable resistance to studies in India and Indonesia [6, 12, 15]. P. aeruginosa isolates were 100% resistant to ampicillin and ceftazidime and 68% resistant to ciprofloxacin, higher than previous reports from India and Indonesia [6, 12, 16]. Variations may be explained by differences in geography, lifestyle, and health education, as well as by study period and sample size.
Resistance genes were detected among the isolates. Most E. coli isolates harbored blaNDM-5, blaOXA-1, blaTEM-1B, and blaCTX-M-15, conferring resistance to carbapenems, ampicillin, amoxicillin/clavulanic acid, and cephalosporins, consistent with studies from referral hospitals in Tanzania and government clinics in Karaikudi [17, 18]. Additionally, qnrS1 genes, conferring quinolone resistance, and aac(3)-IId, conferring aminoglycoside resistance, were identified, aligning with previous reports [17–19]. Among K. pneumoniae, blaSHV and blaTEM were detected [20–22]. S. aureus isolates harbored the aacA-aphD gene, similar to observations from Pakistan [23]. These resistance genes likely contributed to the observed antimicrobial resistance patterns.
Antimicrobial resistance is particularly concerning in patients with diabetes mellitus due to immune compromise, poor glycemic control, bladder dysfunction, and vascular complications [16, 24]. The aminoglycoside resistance observed in this study may be attributed to the detected resistance gene, highlighting the need for routine molecular diagnostics in hospital laboratories to complement phenotypic testing and guide precision antibiotic therapy.
This study has limitations. Convenience sampling may not fully represent diabetic patients in other regions of Tanzania, as the findings reflect the characteristics of patients seeking care at Benjamin Mkapa Hospital. Future studies should include multiple hospitals in Dodoma to provide a more comprehensive understanding of antimicrobial-resistant pathogens in diabetic patients with UTIs.
CONCLUSION
This study demonstrates a high burden of multidrug-resistant (MDR) uropathogens among diabetic patients with urinary tract infections at Benjamin Mkapa Hospital, Tanzania. Escherichia coli, Staphylococcus aureus, coagulase-negative staphylococci, Klebsiella pneumoniae, and Pseudomonas aeruginosa were the predominant isolates, with E. coli being the most frequent. All isolates exhibited resistance to two or more antibiotics, with particularly high resistance to ceftazidime, amoxicillin/clavulanic acid, ciprofloxacin, and ampicillin. At the same time, susceptibility remained higher for meropenem, amikacin, imipenem, and piperacillin–tazobactam.
Genotypic analysis identified clinically important resistance genes, including blaNDM-5, blaOXA-1, blaTEM-1B, blaCTX-M-15, qnrS1, aac(3)-IId, blaSHV, and aacA-aphD, which likely contribute to the observed resistance patterns. These findings highlight the urgent need for routine culture and susceptibility testing, integrated molecular diagnostics, and targeted antibiotic stewardship programs to guide effective therapy and limit the spread of resistant pathogens in this high-risk population.
Despite the study’s limitations due to convenience sampling, the results emphasize the need to expand surveillance across multiple hospitals in Dodoma to achieve a more comprehensive understanding of antimicrobial resistance among diabetic patients with UTIs.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| DM | = Diabetes Mellitus |
| KIA | = Kligler Iron Agar |
| MHA | = Mueller–Hinton Agar |
| TSR | = Template Suppression Reagent |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for this study was obtained from the National Institute of Medical Research (NIMR) Institutional Review Board, reference number Reference No. NIMR/HQ/R.8a/Vol.IX/4640 dated 30 May 2024.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants prior to urine sample collection for bacterial culture and antimicrobial resistance analysis. All patient identifiers were removed and isolates were anonymized before analysis. No identifiable personal data is included in this manuscript.
AVAILABILITY OF DATA AND MATERIALS
The novel blaCTX-M-15 nucleotide sequence generated during this study is available in the NCBI GenBank repository at https://www.ncbi.nlm.nih.gov/genbank/, reference number SUB16174602. Sequences for the remaining genes showed 100% identity to publicly available sequences in GenBank and were therefore not deposited, in accordance with GenBank policy. All other data are contained within the article.
ACKNOWLEDGEMENTS
The authors are grateful to the staff of the Multipurpose Laboratory of the University of Dodoma, Tanzania and the staff of Benjamin Mkapa Hospital, Tanzania, especially the department of the diabetic mellitus clinic, Tanzania for their support in the preparation of the manuscript.
APPENDIX
| Target Gene | Primer Name | 5'-3' Sequence | Source |
|---|---|---|---|
| aac(3)-IId | aac(3)-IIdF | TGA AAC GCT GAC GGA GCC TC | List of primers for detection of antimicrobial resistance genes - version 06.11.2018 |
| aac(3)-IIdR | GTC GAA CAG GTA GCA CTG AG | ||
| blaCTX-M | CTXM1-F3 | GAC GAT GTC ACT GGC TGA GC | |
| CTXM1-R2 | AGC CG C CGA CGC TAA TAC A | ||
| blaNDM-5 | NDM-5-F | GCTCTAGAATGGCTCCAGATGACAAACAT | |
| NDM-5-R | GCTCTAGATGGGTCGAGGTCAGGATAGG | ||
| blaOXA-1 | OXA-1F | ATGAAAAACACAATACATATCAACTTCGC | |
| OXA-1R | GTGTGTTTAGAATGGTGATCGCATT | ||
| blaTEM | TEM-F | ATGAGTATTCAACAT TTC CG | |
| TEM-R | CCAATGCTTAATCAG TGA GG | ||
| qnrS1 | QnrS1-F | ATTATTTGTTACAGACCCGG | |
| QnrS1-F | GCTAACTTTGCAACAGTGCC | ||
| aacA-aphD | aacA-aphD F | TAA TCC AAG AGC AAT AAG GGC | |
| aacA-aphDR | GCC ACA CTA TCA TAA CCA CTA | ||
| blaSHV | SHV-F | TTCGCCTGTGTATTATCTCCCTG | |
| SHV-R | TTAGCGTTGCCAGTGYTCG |
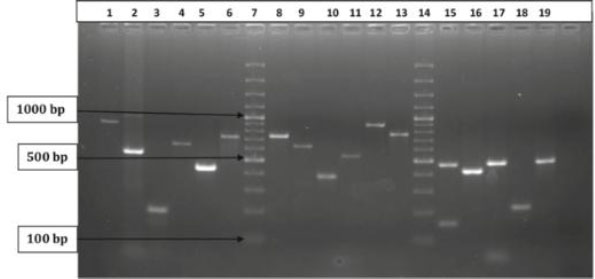 |
Agarose gel electrophoresis of PCR products with representative E. coli isolates carrying the various tested resistant genes. Lane 1: blaTEM (867 bp), lane 2: blaCTXM (540 bp), lane 3: blaOXA-1 (198 bp), lane 7, 14: 100 bp plus ladder, lane 8: aac(3)-IId (740 bp).

