All published articles of this journal are available on ScienceDirect.

Probiophage: A Novel Candidate for the Treatment of Irritable Bowel Disease (IBD): A Systematic Review
Authors Info & Affiliations
Abstract
Introduction
Inflammatory Bowel Disease (IBD), including Crohn’s disease and ulcerative colitis, is a chronic condition characterized by gastrointestinal inflammation, leading to symptoms such as abdominal pain, fatigue, diarrhea, weight loss, and rectal bleeding. While the exact etiology of IBD remains unclear, factors such as immune dysfunction, genetic predisposition, and gut microbiota dysbiosis play significant roles.
Methods
Current treatments include medications and surgeries, but these often fail to address the underlying microbial imbalances. Research highlights that IBD patients frequently exhibit reduced gut microbiota diversity and an overgrowth of pathogenic bacteria.
Results
Probiotics, such as Lactobacillus rhamnosus GG and Escherichia coli Nissle 1917, have shown promise in alleviating symptoms, while bacteriophages are emerging as a novel therapeutic option. This systematic review explores the concept of probiophages, a synergistic combination of probiotics and bacteriophages, as a potential breakthrough in IBD treatment. We examine the roles of gut microbiota, bacteriophages, and probiotics in IBD pathogenesis and therapy, focusing on their combined effects in restoring microbial balance and reducing inflammation.
Discussion
Despite promising preclinical and clinical findings, further research is needed to optimize probiophage formulations, validate their efficacy, and ensure long-term safety.
Conclusion
This review underscores the importance of advancing probiophage-based therapies as a safer and more effective alternative to conventional IBD treatments, addressing the urgent need for innovative approaches in managing this complex disease.
1. INTRODUCTION
IBD is a term used for chronic inflammation of the Gastrointestinal Tract (GIT). Different conditions like Crohn’s disease and ulcerative colitis are associated with long-term (chronic) inflammation that damages the GIT [1]. IBD is commonly characterized by symptoms, such as abdominal pain, fatigue, persistent diarrhea, weight loss, and Rectal bleeding.
The genetic burden of IBD has surged, with 6.8 million cases worldwide in 2023. Prevalence is highest in North America and Europe (0.5%), but incidence is rising rapidly in Asia, South America, and Africa due to urbanization, dietary shifts, and better diagnostics. Genetic factors (e.g., NOD2, IL23R) and environmental triggers (Western diets, smoking, antibiotics) contribute to IBD. Climate change, including rising temperatures and air pollution, is increasingly linked to gut inflammation and dysbiosis [2, 3].
The cause of IBD is unknown, and there are various factors, like the immune system and genetic components. Microbial agents, especially viruses or bacteria, which cause inflammation of the GIT, can lead to IBD. Additionally, genetic elements can relate to IBD. Inappropriate immune response is more likely to develop in patients with a family history [4].
Diagnosis of IBD relies on a combination of clinical evaluation, imaging, endoscopy, histopathology, and laboratory tests. Endoscopy (colonoscopy and upper endoscopy) remains the gold standard for visualizing mucosal inflammation and obtaining biopsy samples [3]. Imaging techniques such as MRI and CT enterography are used to assess disease extent and complications [5]. Serological markers like C-Reactive Protein (CRP) and fecal calprotectin are non-invasive tools for monitoring disease activity [6]. Advances in genotypic approaches, including Next-Generation Sequencing (NGS) and PCR, have enabled the identification of microbial and genetic biomarkers associated with IBD [7]. Additionally, fecal microbiota analysis is increasingly used to assess dysbiosis and guide personalized treatment strategies [7].
The gut microbiota in patients with IBD undergoes significant changes, known as dysbiosis, which may contribute to the developing of disease states. It is uncertain whether dysbiosis is a cause or a consequence of immune activation and inflammation in IBD [8]. Various factors, such as dietary changes, environmental shifts, infections, medications, and lifestyle choices, can disrupt the stability of the gut microbiota. In response to IBD dysbiosis, the host releases antimicrobial peptides, immune mediators, and other elements to restore the balance in host-microbe relationships. Studies have shown that the microbiota in IBD patients has reduced diversity and increased in less abundant phyla. However, the lack of important clinical data and reliance on low-resolution sequence analytics have limited mechanistic insights [9, 10]. More informative approaches, such as metagenomics, metatranscriptomics, and metabolomics, in conjunction with host metadata, are being increasingly utilized [11, 12]. Furthermore, the application of open-source analysis and machine-learning platforms can aid in the integration and analysis of complex datasets. For instance, a study accurately predicted the development of colitis in mice based on metagenomic signatures of antibiotic-induced dysbiosis [13-15].
Available and approved therapies for IBD are 5-aminosalicyclic acids, immunomodulators, and corticosteroids. However, in some patients, there is a need for surgeries to remove damaged portions of the gastrointestinal tract [16].
Despite advances in IBD therapy, including the use of biologics (e.g., anti-TNF agents) and immunomodulators, many patients experience incomplete responses or adverse effects [5]. Antibiotics, while effective in certain cases, can exacerbate dysbiosis and contribute to antimicrobial resistance [7]. There is a pressing need for novel therapies that target the underlying causes of IBD, particularly gut microbiota dysbiosis, without compromising the host's microbial balance [6, 7].
While numerous scientific studies support the potential effect of probiotics in IBD, there needs to be more clinical trial data. The use of probiotics as additional treatments for IBD was advised, given their safety and overall tolerance. However, their effectiveness is enhanced when used alongside other therapies. It is important to note that not all probiotics are the same, and their efficacy varies for different conditions within IBD. Probiotics have various hypothesized mechanisms of action, including direct antimicrobial activity, impact on gut barrier integrity, and immune activity. Well-designed randomized clinical trials are crucial to evaluating probiotics' efficacy in IBD. Ongoing studies in Canada and the European Union are expected to provide rigorous clinical trial data to advance the probiotic field [17].
Research in the probiotics industry is necessary for dose-ranging and comparison studies. Regulatory oversight is limited, and the accuracy of bacterial levels in products is uncertain. Promising probiotics for addressing IBD include L. rhamnosus GG, E. coli Nissle 1917, S. boulardii, and VSL#3. Further investigation is required in pouchitis and mild-to-moderate ulcerative colitis, comparing probiotics to antibiotics, and exploring their combination with other therapies. Additionally, the potential of probiotics in reducing colon cancer risk should be evaluated in high-risk patients [17-19]. Traditional therapies such as antibiotics and probiotics have limitations. Antibiotics can lead to dysbiosis and resistance, while probiotics may not always effectively colonize or target specific pathogens. Probiophages, which are bacteriophages used in combination with probiotics, offer a targeted approach to modulate the gut microbiota by eliminating harmful bacteria and preserving beneficial bacteria [20]. The use of probiotics is justified by their ability to precisely target and destroy pathogenic bacteria, potentially reducing inflammation and improving gut health without disrupting the beneficial microbiota [20, 21]. This approach could be superior to traditional therapies because it avoids the effects of broad-spectrum antibiotics and enhances the efficacy of probiotics by creating a more favorable environment for colonization [20, 21]. Antibiotics, for example, are effective in modulating the gut microbiota, but they can lead to dysbiosis and antibiotic resistance. Probiophages prevent these issues by targeting specific pathogens. Probiotics can modulate the gut microbiota, but may not always effectively colonize or persist in the gut environment [20, 21]. Probiophages can enhance the effect of probiotics by reducing competition from harmful bacteria [20, 21].
The purpose of this article is to review the emerging role of probiophages, a combination of probiotics and bacteriophages, in the treatment of Inflammatory Bowel Disease (IBD). We aim to provide a comprehensive overview of the current understanding of gut microbiota dysbiosis in IBD, the therapeutic potential of bacteriophages and probiotics, and the synergistic effects of combining these therapies. Additionally, we discuss the challenges and future directions for developing probiophage-based treatments for IBD.”
2. METHOD
2.1. Search Strategy
This review adhered to the PRISMA 2020 Flow Diagram (Fig. 1). A comprehensive search strategy was employed to identify valid articles published from 2010 to 2023 across multiple databases, including PubMed, Scopus, and Google Scholar. Standard keywords were extracted from MeSH and used to search for relevant studies. The review involved parallel searches by three researchers to ensure thoroughness. Studies involving patients with Inflammatory Bowel Disease (IBD), including Crohn’s Disease (CD) and Ulcerative Colitis (UC), or animal models of IBD were included.
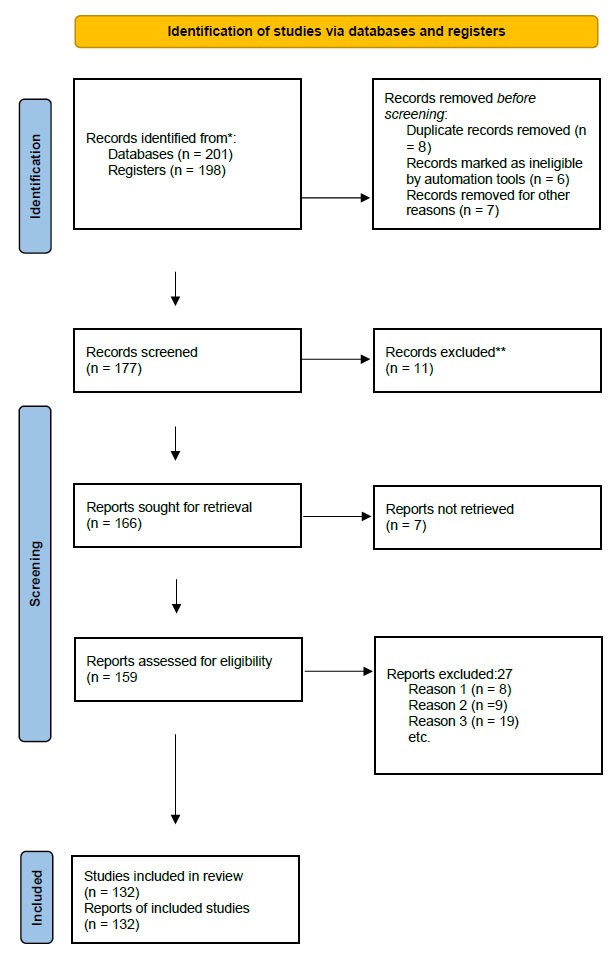
PRISMA 2020 Flow Diagram. Flowchart illustrating the study selection process for this systematic review, adapted from the PRISMA 2020 guidelines (Reason 1: No full text (Abstract), Reason 2: Non-English, Reason 3: Insufficient Size, Unmet Criteria).
| Element | Description |
|---|---|
| P (Population) | Patients with Inflammatory Bowel Disease (IBD), including Crohn’s disease and Ulcerative Colitis; animal models of IBD; preclinical and clinical human studies related to IBD. |
| I (Intervention) | Probiophage therapy (combination of probiotics and bacteriophages) and bacteriophage therapy targeting gut microbiota dysbiosis in IBD. |
| C (Comparison) | Placebo, standard care, probiotics alone, antibiotics, or no intervention, depending on individual studies reviewed. |
| O (Outcomes) | Reduction in intestinal inflammation; modulation of gut microbiota composition; improvement in clinical symptoms and mucosal healing; safety and viability of probiophage therapy. |
| S (Study Design) | Systematic narrative review including preclinical animal studies, metagenomic analyses, early-phase clinical trials, and observational studies |
Primary outcomes included reduction in IBD symptoms, improvement in gut microbiota composition, and reduction in inflammatory markers. Secondary outcomes focused on safety, tolerability, and long-term efficacy. The search strategy combined MeSH terms and free-text keywords related to IBD, probiotics, bacteriophages, and biotic therapies. The search strategy was tailored for each database, and no date or language restrictions were initially applied. However, non-English studies were excluded during screening. Titles and abstracts of retrieved records were independently screened by two reviewers to identify potentially relevant studies. Full-text articles of potentially relevant studies were assessed for eligibility based on predefined inclusion and exclusion criteria. Abstracts and articles with insufficient sample sizes were excluded. Studies that did not meet the inclusion criteria were excluded.
The key elements of the included studies on probiophage treatment in inflammatory bowel disease are summarized in Table 1.
3. RESULT
3.1. The Role of Bacteriophages in Modulating Intestinal Microbiota in IBD
The association between bacteriophages and the intestinal microbiota is an intricate and dynamic relationship that has gained increasing attention in recent years [22]. Bacteriophages, also known as phages, are viruses that specifically infect and replicate within bacterial cells. Bacteriophages are the most plentiful and diverse biological entities in the human gut, and have a vital impact on shaping the composition and function of the intestinal microbiota [23].
The gut microbiota is a diverse community of trillions of microorganisms, such as bacteria, viruses, fungi, and other microbes, that reside in the human gastrointestinal tract [24]. This complex ecosystem greatly affects human health by influencing immune function, metabolism, and the onset of different diseases. Bacteriophages have been shown to have a significant impact on the composition and dynamics of the intestinal microbiota [25]. They can directly affect the abundance and diversity of bacterial species by infecting and eliminating specific bacterial strains, thus influencing the overall balance of the microbiota. Furthermore, bacteriophages can facilitate the transfer of genetic material between bacteria, resulting in the dissemination of antibiotic resistance and other advantageous or detrimental traits within the microbiota [21, 26]. Furthermore, bacteriophages have been implicated in regulating host-microbe interactions and immune responses in the gut. They can influence the activity of the immune system and the production of antimicrobial peptides, thus shaping the overall health of the host [27]. Understanding the intricate interplay between bacteriophages and the intestinal microbiota is crucial for developing novel therapeutic strategies to modulate the microbiota and treat various diseases. Research in this field is rapidly advancing, and it holds great promise for improving our understanding of the gut microbiome and its impact on human health.
3.2. Different Types of Phages and Their Therapeutic Mechanisms
Three key characteristics are used to classify bacteriophages: their morphology, genetic composition, and life cycle [28]. The Caudovirales order, with its long, non-enveloped tails, is the most extensively studied morphology. This family is further divided into the Myoviridae, Podoviridae, and Siphoviridae families, each with its unique tail structure (Table 2). Filamentous bacteriophages have their genetic material enclosed in a protein coat, which is a crucial part of their long, flexible, filament-like structures [29].
Tectiviridae are distinguished by their icosahedral head surrounded by a tectiviral-like lipid membrane [33]. The genetic material is encapsulated in long, flexible, helical structures called Inoviridae, which contain icosahedral [34]. The tiny RNA phages, called Levividae, are composed of an icosahedral capsid that contains a single-stranded RNA genome [33]. The minuscule, non-enveloped Microviridae have an icosahedral capsid enclosing a single-stranded DNA genome [33]. Pleolipoviridae are pleomorphic, meaning their envelopes contain lipids and they can have filamentous, spherical, or irregular morphologies [35]. When it comes to genomic characteristics, RNA phages can have genomes based on double-stranded RNA (dsRNA) or single-stranded RNA (ssRNA), whereas DNA phages can have genomes based on either type of DNA [36].
| Family | Structural Features | Morphology | Examples |
|---|---|---|---|
| Myoviridae | - Icosahedral capsid - Thick, contractile tail with sheath - Prominent baseplate - Long and short tail fibers - Whiskers - Collar |
Large, complex phage with robust, contractile tail; tail sheath contracts during infection | Phage T4 (infects E. coli) Phage OMKO1 (P. aeruginosa) [30] Lactobacillus phages (Semelevirus) [31] |
| Siphoviridae | - Icosahedral capsid - Long, thin, non-contractile tail - Simple baseplate - Tail fibers - Collar |
Slender, flexible tail; non-contractile; simple attachment apparatus | Phage λ (lambda, infects E. coli) Enterococcus phage IME-EFm5[REMOVED HYPERLINK FIELD] [32] |
| Podoviridae | - Icosahedral capsid - Short, stubby tail - Minimal tail fibers - Simple baseplate |
Short, rigid tail; minimalistic tail structure; compact appearance | Phage T7 (infects E. coli) Phage P22 (Salmonella) [30-32] |
Based on their life cycle, bacteriophages are divided into two groups: the lysogenic phages and the lytic phages. Pseudo-lysogenic, or temperate phages, can be lytic, killing host cells, or lysogenic, going dormant in the host after integrating into the host's DNA [37-39]. Lytic phages reproduce inside their host cell, eventually causing cell lysis and the release of daughter phage particles. These are known as virulent phages [40].
Phage treatments, which target harmful and opportunistic microorganisms in the stomach that can cause illness, are currently in development. These treatments, which can be combined with probiotics and antibiotics, include single phages, cocktails, and genetically engineered phages. Research is focused on creating treatments for common gut-infecting bacteria such as Salmonella spp., Fusobacterium nucleatum, Escherichia coli, Clostridioides difficile, Listeria monocytogenes, Ruminococcus gnavus, and Vibrio spp. Many bacteriophage species may be utilized in this field as effective therapeutic substitutes for dealing with drug-resistant strains [41, 42].
3.3. Phage Therapy and IBD
Inflammatory Bowel Diseases (IBDs) are auto-inflammatory disorders characterized by an unregulated innate and adaptive immune response, leading to persistent tissue destruction [43]. These disorders encompass Ulcerative Colitis (UC), Crohn's Disease (CD), and indeterminate colitis [44].
Intestinal inflammation is a complex condition that is influenced by the gut microbiota. Studies have demonstrated that transferring dysbiotic IBD-associated microbiota into healthy mice can induce intestinal inflammation. Conversely, in animal models susceptible to IBD, intestinal inflammation is alleviated by depleting the microbiota through antibiotic treatment. This indicates that the composition of the microbiota is a critical factor in the development and advancement of intestinal inflammation [43, 45, 46].
It is believed that the presence of pathobionts such as Multi-Drug Resistant (MDR) Klebsiella pneumoniae, Adherent-Invasive E. Coli (AIEC), Enterococcus faecium, enterotoxigenic Bacteroides fragilis, or others can exacerbate IBD in genetically susceptible hosts [47]. However, the use of broad-spectrum antibiotics for IBD in humans is still a topic of debate and has been associated with side effects, dysbiosis, and the development of resistant strains [48]. A challenging and unresolved issue is the long-term, specific elimination of IBD-related pathobionts without impacting the surrounding microbial community. The effectiveness of Fecal Microbiota Transplantation (FMT) in UC and CD varies; certain studies have even documented FMT-linked worsening of the disease [49].
Bacteriophages are ubiquitous, self-replicating viruses that bind to specific bacterial receptors to infect bacteria with a high level of host specificity [50]. Bacteria have developed a multitude of anti-phage defense mechanisms through an ongoing “arms race,” including restriction endonucleases, CRISPR, and a variety of recently discovered systems whose mechanisms are still being revealed [51, 52]. Phage therapy has recently gained attention for its potential as a rescue treatment against Multi-Drug-Resistant (MDR) infections. However, its usage is limited to the short term due to human immunity and bacterial resistance [53, 54]. Klebsiella pneumoniae has been found to be highly correlated with the severity of IBD in four geographically varied cohorts of patients with IBD (n = 537). In mouse IBD models, K. pneumoniae colonization caused gut inflammation, which was reduced when a specific K. pneumoniae-targeting five-phage cocktail was administered. Finally, proof-of-concept tests in a human-like artificial gut and healthy subjects demonstrated the safety and viability of phage therapy [47].
3.4. Biotics and Intestinal Microbiome
The human gut is a complex ecosystem comprising over 1,000 species of bacteria and other microorganisms, which may outnumber the host cells [55, 56]. Its main role is to support the digestive system, but it also performs other functions, such as vitamin production and regulation of the immune system. Additionally, by stimulating the intestinal epithelium, it also influences the host’s behavior [57, 58]. The host and the microbiome engage in two-way communication. By identifying host peptides and hormones, the microorganism ensures that it is in an appropriate situation and increases the expression of genes associated with colonization. Conversely, microorganisms in other compartments produce metabolite signal molecules that aid in the maturation of the immune system and influence immune homeostasis and mucosal integrity [59]. For example, metabolites of tryptophan and short-chain fatty acids play a role in affecting intestinal disorders, particularly the pathogenesis of IBD [60]. The microorganisms residing in the intestinal tract have both positive and negative effects, and this microbial population changes due to illness and diet. Among the beneficial effects of microorganisms are the prevention of bacterial invasion and the synthesis of nutrients and essential substances [61-63]. Microorganisms with positive effects can be utilized as supplements to enhance health. In addition to probiotics, there is now a new category known as biotics, which will be discussed in detail [64].
3.5. Types of Biotics and Their Therapeutic Mechanisms of Action
3.5.1. Probiotics
The first recorded use of probiotics as a treatment for infections or food poisoning dates back to ancient China. According to the latest definition, probiotics are living organisms that, if they reach the intestine in sufficient quantities, contribute to intestinal homeostasis [65]. Different strains work in different ways, but one method is by producing antibacterial substances such as lactic acid, hydroperoxides, and bacteriocins. They also block binding sites in epithelial cells and upregulate tight junction molecules in the mucosal barrier [66-68]. Lactobacillus and Bifidobacterium genera are some of the most well-known and commonly used probiotic strains, and they continue to be widely utilized in the production of nutritional supplements. Many individuals have strains of Faecalibacterium prausnitzii, Akkermansia muciniphila, and Clostridia in their gut microbiota, which are known as next-generation probiotics. Research has shown that a decrease in these bacteria in the gut microbiome can increase the likelihood of developing immune-metabolic diseases such as obesity, type 2 diabetes, and Multiple Sclerosis (MS) [69, 70]. Several mechanisms have been proposed for the therapeutic effect of probiotics. They prevent the adhesion of pathogenic bacteria, and some also have competitive exclusion properties by adhering to the intestinal mucosa to prevent further attachment of pathogens. For instance, specific strains of Lactobacillus have been shown to inhibit the adhesion of pathogens such as Enterotoxigenic E. Coli (ETEC) to porcine enterocytes, diarrheagenic E. coli to Caco-2 cell lines from the human intestinal epithelium, and Salmonella typhimurium to intestinal cell lines [71-73]. The following mechanism enhances intestinal barrier function. A hyperpermeable epithelial barrier in the gastrointestinal tract is suspected to be the primary cause of chronic inflammation. Probiotics improve the structure and function of the gut's epithelial barrier by increasing mucin and Short-Chain Fatty Acid (SCFA) production, improving tight junctions, and modulating signaling pathways that affect cell proliferation and survival. Additionally, probiotics can alter the innate and adaptive immune systems. They accomplish this by interacting with receptors of the innate immune system, such as Toll-Like Receptors (TLRs), which are present on intestinal epithelial cells and mucosal immune cells. Additionally, they have the ability to modify important signaling pathways, including NF-κB, mitogen-activated protein kinase, phosphoinositide-3-kinase protein kinase B/Akt (PI3K-PKB/Akt), and Peroxisome Proliferator-γ (PPAR-γ) [74]. Moreover, probiotics are taken up by Dendritic Cells (DCs) and contribute to the promotion of DC maturation and induction of regulatory T cells (Tregs). Tregs play a crucial role in establishing immune homeostasis and maintaining tolerance [75, 76]. Probiotics can also stimulate the production of anti-inflammatory cytokines, such as Transforming Growth Factor (TGF)-β and IL-10, while reducing the secretion of pro-inflammatory cytokines like interleukin IL-8, TNF-α, and Interferon gamma (IFN-γ) [77].
3.5.2. Prebiotics
Prebiotics are indigestible dietary fibers that impact a person’s health by stimulating the activity or growth of intestinal microorganisms [78]. They are non-absorbable and seldom cause adverse effects. A prebiotic should: 1. resist acidic conditions of the stomach and digestive enzymes; 2. not be absorbed by the digestive system; 3. be fermentable and consumed by the intestinal microbiota [79]. Prebiotics can be artificially produced and added to supplements and food products to enhance nutritional value and health. They are also found in many plant-based products such as artichokes, garlic, onions, wheat, and bananas. They increase the number of beneficial bacteria in the human intestinal tract, including families of Lactobacillaceae, Bifidobactericeae, and Bacteroidaceae [80]. The most common prebiotics include inulin, Glycooligosaccharides (GOS), Fructooligosaccharides (FOS), lactulose, galactose, and glucan derivatives [80, 81]. Consumption of prebiotics has been shown to enhance the immune function of the host, reduce infection rates, improve colon integrity, and down-regulate allergic reactions. SCFAs have beneficial effects on GI disorders through several mechanisms. They inhibit the growth of pathogens, accelerate the proliferation of beneficial bacteria due to their loose structure and large surface area, and increase the production of SCFAs, including acetate, butyrate, and propionate. These SCFAs are produced during the fermentation of prebiotics and are crucial for the proper functioning of the intestine. They support the regeneration and healing of intestinal epithelial cells, enhance mucus production, and help maintain the correct pH in the intestine. Additionally, they prevent the attachment of pathogenic microorganisms to intestinal cells [77].
3.5.3. Synbiotics
Gibson first introduced the concept of probiotics approximately 25 years ago and proposed the added advantages of combining probiotics and prebiotics, resulting in the development of synbiotics. Synbiotics consist of a combination of probiotics and prebiotics. In essence, prebiotics are “nutrients” recognized as functional food components for probiotics, which can benefit the host by synergistically enhancing the survival and activity of “good” microorganisms in the large intestine [78, 82, 83]. Probiotic strains in synbiotic formulations include Lactobacillus spp., Bifidobacterium spp., Saccharomyces boulardii, and Bacillus coagulans. In contrast, the main probiotics used include oligosaccharides such as Fructo-Oligosaccharide (FOS), GOS, Xylose-Oligosaccharides (XOS), prebiotics, and natural roots. According to previous studies, the benefits of using synbiotics by humans include: increasing the levels of Lactobacillus spp, Bifidobacterium spp, and Saccharomyces boulardii, as well as balanced intestinal microbiota; improving liver function in cirrhosis patients; improving the ability to modulate immunity; and preventing bacterial transmission in non-acidic patients [84]. The synergism of probiotics and prebiotics selectively promotes the growth of microbes or activates specific metabolic processes through the gut microbiota. Synbiotics have a significant impact on reducing the expression of TNF-α, a pro-inflammatory cytokine, and therefore may be beneficial in managing GI disorders. Additionally, synbiotics may have positive effects on the intestinal mucosa [77].
3.5.4. Paraprobiotics
The term paraprobiotic was first introduced in 2011 [85]. Paraprobiotics consist of non-living, inactive bacterial strains, bacterial fragments, and their metabolites. Due to the potential risks associated with live probiotics for certain individuals, such as those with immune system deficiencies, premature infants, and sepsis, the use of paraprobiotics can be beneficial [86, 87]. Paraprobiotics are easier to produce and store because they are non-living and have a predictable mechanism of action. Some advantages of using paraprobiotics include the absence of risk in transferring antibiotic-resistance genes and preventing disease in at-risk individuals caused by live microorganisms. Additionally, paraprobiotics allow for easy production and transportation, as well as the creation of commercial products through bacterial strain cultivation and inactivation [88-90]. Bacterial species that are particularly important for promoting human health, known as paraprobiotics, include Bifidobacterium lactis Bb12, Bifidobacterium longum, Lactobacillus gasseri OLL2716, Saccharomyces cerevisiae, Lactobacillus brevis SBC8803, and Lactobacillus delbrueckii subsp. Bulgaricus OLL1073R-1 [88]. The most important mechanism of parabiotics is immunomodulation. A study has shown that they reduce the expression of monocyte chemoattractant protein-1 (MCP-1) (p < 0.05) and regulate the expression of TNF-α and IL-12 (p < 0.05) in an in vitro model of intestinal mucositis using Caco-2 cells and inactivated L. rhamnosus [91]. Likewise, it has been shown that they have anti-inflammatory properties and can suppress pro-inflammatory cytokine production [92, 93].
3.5.5. Postbiotics
The term postbiotics refers to metabolites, Cell-Free Supernatants (CFS), and soluble factors (metabolic by-products or products) secreted by living bacteria [94]. Postbiotics are found in many foods, such as kefir, yogurt, and pickles, as well as in the human body. Organic acids, SCFA, tryptophan (Trp), and bacteriocins can be mentioned among the essential postbiotics [95]. According to the type of microorganism, strain, and metabolite, they have different effects. Their mechanisms of action are direct and indirect. Direct effects are applied directly to the host cell. Indirect effects are implemented by increasing the growth of beneficial bacteria and inhibiting the growth of pathogenic bacteria [96]. Postbiotics may be beneficial in managing GI disorders through several potential effects, including anti-inflammatory, antibacterial, immunomodulatory, anti-cancer, anti-oxidant, anti-hypertensive, anti-proliferative, and cholesterol-lowering properties. Several mechanisms of action have been proposed, some of which include inhibiting the production of IL-12, reducing the level of cyclooxygenase-2 (COX-2) and nitric oxide synthase (iNOS), reducing the expression of IL-6, TNF-α, and IL-1β, modulating the NF-κB pathway, and PPARγ [97].
4. DISCUSSION
4.1. Biotic Therapy and IBD
Studies have shown that administering antibiotics to reduce IBD-associated microbial concentration can lead to adverse changes in the intestinal microbial population [98]. Therefore, based on the current understanding of IBD pathogenesis, antibiotic treatment does not always result in a positive outcome [99]. The rapid advancement of molecular and metagenomics studies has not only facilitated the understanding of how IBD begins, but has also generated new treatment concepts [100]. One of these new treatment strategies is biotics, which target the intestinal microbiome to reduce the development of IBD and restore dysbiosis [101].
In numerous studies, a reduction in probiotics, such as Bifidobacterium and Lactobacillus spp., was observed concurrently with the abnormality of the intestinal microflora in IBD patients. Oral administration of probiotics is widely utilized to enhance the condition of intestinal microflora in various intestinal disorders [102, 103]. The efficacy of probiotics varies in clinical and animal studies due to the diversity in microorganism type, dosage, frequency, and duration of use. In general, one or multiple probiotic strains have been utilized as treatments in various studies. For instance, the commercial probiotic VSL#3, which comprises eight bacterial strains, is among the most commonly used probiotics in humans. Conversely, the efficacy of using a single strain of Bifidobacterium breve CCFM683 for intestinal microbial recovery has been documented in a C57BL/6J mouse model [104-106]. The probiotics' dosage is crucial; commercial supplements contain 1-10 × 10 9 CFU in each dose, which is indeed the necessary number of microorganisms for the effectiveness of a probiotic supplement [107]. As per various studies, it has been suggested that the duration of probiotic therapy should be at least seven days [108]. Additionally, some studies have suggested that probiotic therapy should be administered for a minimum of one year to evaluate its health effects [104]. The most common probiotic strains used in animal studies and clinical trials belong to the Lactobacillus and Bifidobacterium genera [108, 109]. Furthermore, other bacterial strains that have been evaluated for their probiotic potential include Escherichia coli Nissle 1917 [110], Clostridium butyricum [111], Weissella paramesenteroides WpK4 [112], and Saccharomyces boulardi [113]. Among the commercial supplements utilized in various clinical trials for treating IBD, supplement VSL#3 comprised a group of eight distinct probiotic strains, including Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus casei, Lactobacillus delbrueckii subspecies bulgaricus, Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium infantis, and Streptococcus salivarius subspecies thermophilus, which have the most effectiveness, according to the published data [104, 114-117]. According to previously published review articles, this commercial supplement, which possesses various health regulation mechanisms, has been extensively used to treat UC and other symptoms of IBD by restoring the gut microflora, reducing inflammation, and reducing microbial transmission [106, 116, 117]. Tursi et al. (2010) reported significant UC treatment using the VSL#3 probiotic supplement compared with placebo [106]. The results of the first evaluation of Clostridioides difficile recurrence prevention by Fedorak et al. (2015) showed that the long-term use of VSL#3 is associated with promising results for reducing IBD [104].
Surprisingly, there have been more animal studies on the use of prebiotics in treating IBD than in human clinical trials; however, prebiotics are associated with the flourishing of beneficial gut microbiota and resistance to pathogenic microorganisms [118, 119]. Prebiotics used in animal studies include polysaccharides extracted from vegetables such as kale and fruits such as grapes and gooseberries [119, 120]. However, in human clinical trials, prebiotic fructo-oligosaccharides have often been used to treat patients with IBD [107, 121]. The data obtained from studies that have used inulin supplements enriched with fructo-oligosaccharides show that the production of butyrate and acetylide occurs at a higher level, followed by an increase in beneficial microbial populations such as Lactobacillus and Bifidobacterium [118, 122]. Data from these studies indicate the consumption of 2.5-15 grams of FOS per day [121-123]. In 2015, Azpiroz et al. reported that increased doses of FOS supplements were associated with an increase in intestinal bifidobacteria, and other studies also showed a positive effect of FOS on the increase in other butyrate-producing bacteria [122, 124, 125].
As was already said, synbiotics are products that contain both probiotics and prebiotics. They work together to improve the condition of the intestine in a way called synergistic action [119, 126]. In animal studies and clinical interventions, the administration of synbiotics has been used to treat IBD and has been shown to significantly reduce inflammation [114]. A placebo-controlled clinical trial showed that a synbiotic treatment with six types of probiotics and FOS as a prebiotic reduced inflammation in the intestines and improved the disease more than the control group [114]. In 2021, Liang et al. used a synbiotic to reduce the symptoms of diarrhea associated with IBD in a randomized, double-blind, placebo-controlled clinical trial. The results indicated significant improvement in the feeling of incomplete bowel movements, pain in the rectum, bloating, and diarrhea [127].
Postbiotics are compounds obtained from microbial fermentation, and their efficiency varies depending on the type of molecule or metabolite [128, 129]. Their effectiveness can be related to the effect on the composition of the microflora and the health of the host. Postbiotics have been used to treat IBD in several animal models and cell line-based studies [130-132]. For example, a study has shown that E. coli EcN1917 produces more hydroxyoctadecaenoic acid (C18-3OH) than other strains. Administering C18-3OH in a murine model of colitis with pseudomembrane leads to recovery and regeneration of intestinal dysbiosis [132]. On the other hand, this treatment method makes it possible to combine different bioactive components to accelerate the healing process.
4.2. Bacteriophage-biotic Cocktail (Probiophages)
The bacteriophage cocktails can target specific disease-causing bacteria, whereas probiotics help rebalance the microbiota for improved health outcomes. Together, they provide a synergistic approach to managing difficult-to-treat bacterial infections in the gut, skin, oral cavity, and other sites [7]. There has been growing interest in developing phage-probiotic combination approaches as a new treatment strategy for IBD, including UC and CD [133]. Several studies have explored the combination of bacteriophages targeting pathogenic bacteria, such as Escherichia coli, Klebsiella pneumoniae, and Salmonella spp., along with probiotic strains of Lactobacillus, Bifidobacterium, and others, to modulate the microbiome and reduce inflammation [134]. Initial studies in mouse models of chemically induced colitis have demonstrated promising outcomes. Oral administration of an anti-Salmonella phage cocktail combined with Lactobacillus plantarum and Bifidobacterium infantis probiotics significantly attenuated weight loss, colon tissue damage, and inflammatory markers compared with phage or probiotic alone in mice with TNBS-induced colitis [133, 134]. In another study in mouse colitis models, combined phage-probiotic therapy produced more significant anti-inflammatory effects and dysbiosis reversal compared with either intervention alone. This integrated treatment method can restore gut
| Year | Study/Development | Key Findings/Contributions | Therapeutic Approach | Disease Focus | Reference/Author(s) |
|---|---|---|---|---|---|
| 2015 | The probiotic VSL#3 has anti-inflammatory effects and could reduce endoscopic recurrence after surgery for Crohn's disease | VSL#3 showed anti-inflammatory effects and reduced endoscopic recurrence in Crohn's disease | Clinical (human trials) | Crohn's disease | [104] |
| 2017 | Early transcriptomic changes in the ileal pouch provide insight into the molecular pathogenesis of pouchitis and ulcerative colitis | Transcriptomic changes in the ileal pouch linked to pouchitis and ulcerative colitis | Preclinical (animal models) | UC | [14] |
| 2018 | Dynamics of metatranscription in the inflammatory bowel disease gut microbiome | Metatranscriptomic analysis revealed dynamic changes in the gut microbiome in IBD | Preclinical (human studies) | IBD | [13] |
| 2019 | Effects of synbiotic therapy in mild-to-moderately active ulcerative colitis | Synbiotic therapy showed positive effects in managing ulcerative colitis symptoms | Clinical (human trials) | UC | [114] |
| 2020 | Multi-omics of the gut microbial ecosystem in inflammatory bowel diseases | Multi-omics approach revealed insights into the gut microbial ecosystem in IBD | Preclinical (human studies) | IBD | [13] |
| 2021 | Metagenomic alterations in gut microbiota precede and predict the onset of colitis in the IL10 gene-deficient murine model | Metagenomic changes in gut microbiota predict colitis onset in IL10-deficient mice | Preclinical (animal models) | Colitis | [15] |
| 2022 | Phage therapy for Klebsiella pneumoniae in human IBD cohorts | Phage cocktails reduced inflammation in IBD patients with K. pneumoniae colonization | Clinical (human trials) | IBD | [47] |
| 2023 | Phage therapy combined with probiotics (probiophages) in UC | Probiophages showed enhanced anti-inflammatory effects in UC patients compared to placebo | Clinical (human trials) | UC | [127] |
microbiome equilibrium in people with IBD and potentially relieve their symptoms [135]. Moreover, the immune system-modulating characteristics of bacteriophages and the ability of probiotics to enhance IL-10 secretion by gut immune cells indicate a potential immunotherapeutic benefit in the management of IBD. This ability could serve as a means to counteract the heightened levels of IL-1 typically associated with IBD. In addition, phages can reduce the production of Reactive Oxygen Species (ROS), which is connected to the development of IBD. Moreover, phages may induce the production of IL-10, a cytokine crucial for maintaining intestinal equilibrium. Phages can also improve the production of the cytokine interleukin-1 receptor antagonist IL-1RA, which inhibits the pro-inflammatory effects of IL-1 [136]. IL-1RA has demonstrated effectiveness in alleviating intestinal inflammation and experimental colitis. Therefore, the ability of phages to boost IL-1RA production could complement the immunoregulatory benefits of probiotics [136]. As mentioned, dysbiosis and altered diversity of the gut microbiome, along with genetic and immunological factors, are involved in the pathogenesis of IBD [137]. Proposed mechanisms of host-microbiome interactions include bacterial molecules interacting with intestinal cell receptors and transporters, potentially triggering abnormal inflammatory responses in genetically susceptible individuals [137]. Current and potential therapeutic approaches targeting the microbiome are being examined, such as probiotics, fecal microbiota transplants, engineered bacteria that deliver therapeutic molecules, and bacteriophages that target pathogens [137]. Bacteriophages are abundant in the gut, but their influence on IBD requires further research on the dynamics of phage-bacteria [137]. Elucidating microbiome functional dynamics, not just composition, is crucial to clarifying its contributions to IBD and developing improved microbiome-modulating therapies [137].
CONCLUSION
A chronological overview of key studies regarding phage therapy in Inflammatory Bowel Disease (IBD) and Ulcerative Colitis (UC) is presented in Table 3. Our study aligns with existing literature emphasizing the crucial role of gut microbiota in IBD pathogenesis [138]. Both bacteriophages and probiotics have been individually recognized for their potential in modulating gut microbiota, with bacteriophages targeting specific pathogens and probiotics promoting beneficial microbial communities [20, 139]. Traditional treatments for IBD, such as antibiotics and anti-inflammatory drugs, often have significant side effects and may disrupt the balance of gut microbiota, leading to dysbiosis [139]. Our study supports the need for alternative therapies that minimize these risks. Recent advancements in IBD treatment include Fecal Microbiota Transplantation (FMT) and engineered probiotics, which have shown promise in restoring gut balance and reducing inflammation [20, 139]. Our approach with probiophages complements these emerging therapies by offering another tool for targeted microbiome modulation [20, 139]. Additionally, there were Differences from Existing Literature. Unlike previous studies focusing on either bacteriophages or probiotics separately, our research explores the combined use of probiophages [20, 139]. This dual approach may enhance therapeutic efficacy by eliminating harmful bacteria and promoting beneficial microbial growth [20, 139]. While existing literature highlights challenges in phage delivery and specificity, our study investigates novel encapsulation methods and targeted delivery systems to improve the stability and effectiveness of probiophages in reaching the intestinal tract [20, 139]. Our study addresses the gap in understanding how probiophages can be designed to specifically target pathogenic bacteria without harming beneficial microbes, ensuring a safer treatment option compared to broad-spectrum antibiotics [20, 139]. By exploring the long-term stability and efficacy of probiophages, our research contributes to filling the knowledge gap regarding sustained therapeutic effects and the potential for repeated treatments. The current literature often focuses on single therapeutic agents [20, 139]. Our study provides insights into the potential benefits of combining probiotics and bacteriophages, offering a more comprehensive approach to IBD treatment [20, 139].
In conclusion, our research on probiophages for IBD treatment aligns with the broader understanding of gut microbiota's role in disease pathogenesis while introducing a novel combination therapy that addresses existing gaps in specificity, safety, and long-term efficacy [20, 139]. This review highlights the potential of probiophages—a combination of probiotics and bacteriophages—as a novel therapeutic approach for IBD. By targeting dysbiosis and modulating the gut microbiota, probiophages offer a promising strategy for managing IBD symptoms and improving patient outcomes. However, several limitations must be addressed, including the need for large-scale clinical trials, standardized formulations, and long-term safety assessments. Practical recommendations include: conducting multicenter clinical trials, developing guidelines, investigating the impact of environmental factors, and promoting interdisciplinary research to optimize probiophage formulations and delivery methods. By addressing these challenges, probiophages could revolutionize IBD treatment, offering a safer and more effective alternative to existing therapies.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: Study conception and design: AR; Writing the paper: MRM, NN; Validation: RA; Writing- reviewing and editing: AA, MH. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| IBD | = Inflammatory Bowel Disease |
| GIT | = Gastrointestinal Tract |
| CRP | = C-Reactive Protein |
| NGS | = Next-Generation Sequencing |
| Probiophages | = Combination of Bacteriophages and Probiotics |
| CD | = Crohn’s Disease |
| UC | = Ulcerative Colitis |
| MDR | = Multi-Drug Resistant |
| AIEC | = Adherent-Invasive E. Coli |
| FMT | = Fecal Microbiota Transplantation |
| MDR | = Multi-Drug-Resistant |
| MS | = Multiple Sclerosis |
| ETEC | = Enterotoxigenic E. Coli |
| SCFA | = Short-Chain Fatty Acid |
| TLRS | = Toll-Like Receptors |
| PPAR-T | = Peroxisome Proliferator-T |
| DCS | = Dendritic Cells |
| Tregs | = Regulatory T Cells |
| TGF-β | = Transforming Growth Factor β |
| IFN-γ | = Interferon Gamma |
| GOS | = Glyco-oligosaccharides |
| FOS | = Fructo-oligosaccharides |
| XOS | = Xylose-Oligosaccharides |
| MCP-1 | = Monocyte Chemoattractant Protein-1 |
| CFS | = Cell-Free Supernatants |
| COX-2 | = Cyclooxygenase-2 |
| iNOS | = Nitric Oxide Synthase |
| ROS | = Reactive Oxygen Species |
AVAILABILITY OF DATA AND MATERIAL
All the data and supporting information are provided within the article.
ACKNOWLEDGEMENTS
Declared none.

