All published articles of this journal are available on ScienceDirect.

Etiological Agents of Urinary Tract Infection and 7 Years Trend of Antibiotic Resistance of Bacterial Uropathogens in Sudan
Authors Info & Affiliations
Abstract
Introduction:
Bacterial infections of the urinary tract represent a major cause of outpatient visits as well as hospital-acquired infections. As the prevalence of multidrug-resistant uropathogens is increasing, updated knowledge of the commonest bacterial causes and their susceptibility patterns is crucial for the proper selection and use of antimicrobial drugs and the development of effective local prescribing guidelines.
Methods:
Handling of urine samples, identification of organisms and antimicrobial susceptibility testing were made according to guidelines in Monica Cheesbrough 2000, 2006. The prevalence of resistance of the pathogens against each antibiotic was calculated as the proportion of resistant isolates over the entire tested isolates. Data were analyzed using Epi info; the chi-square test and Fisher exact test were used to assess the statistical significance of results.
Results:
In this study, 774 samples were cultured from patients with suspected urinary tract infection (UTI), 705 (91%) urinary isolates showed significant growth (>105 CFU /L) while the other 69 samples showed no significant growth. 431 (61%) of the patients were female, while the other 274 (39%) were males. 13 types of pathogens were identified in 705 urinary isolates. E.Coli was the main bacterial uropathogen identified. Microbiological susceptibility of a total of 28 antibiotics was tested; for each urinary isolate, different sets of these antibiotics were used. 601(96%) of the bacteria were resistant to at least one antibiotic. 17 antibiotics were found to have a bacterial resistance rate of more than 50%, including all B lactams (except cefuroxime), Nalidixic acid, Ciprofloxacin, Norfloxacin, Clindamycin, Co-Trimoxazole and Tetracyclines(Tetracycline and Doxycycline). Other antibiotics were found to have resistance rates of less than 50%. Amikacin & Imipenem had the highest susceptibility rates. Throughout the 7 years, resistance to most of the antibiotics showed an incremental pattern.
Conclusion:
Current empirical antibiotic therapy for UTI should be modified, and new guidelines should be established based on local resistance rates. This study comes up with precious regional data for evidence-based empirical antibiotic treatment, but a national sentinel surveillance system and regional antibiograms should be established to track the bacterial susceptibility profiles in Sudan.
1. INTRODUCTION
Urinary tract infection (UTI) is defined as the colonization of the urinary tract by microbial pathogens. UTIs could be categorized by various methods, anatomically into lower (cystitis), upper (pyelonephritis), or prostatitis. It also can be symptomatic UTI or asymptomatic bacteriuria (ASB). “Uncomplicated” UTI occurs in a normal genitourinary tract with no history of instrumentation while infection in genitourinary tracts that have anatomical, physiological abnormalities or catheterization, is considered “complicated”. [1-3] Bacterial pathogens are the major cause of UTI, accounting for 95% of cases [4].
Analysis of clean-catch urine is commonly used to detect UTIs using rapid screening tests (dipstick leukocyte esterase test or nitrite test) or microscopic examination. Notably, the detection of pyuria is not specific and is not always evidence of clinical UTI. Urine culture is the gold standard test but is not approved for managing uncomplicated lower UTI, such as cystitis. On the other hand, a urine culture and sensitivity test should be obtained for acute pyelonephritis and any type of complicated UTIs, before empiric therapy to optimize the subsequent definitive antibiotic regimen [5].
UTIs are one of the most prevailing bacterial infections with a global incidence of 150 million people /year [6-8]. UTIs have large socio-economic impacts as it ranks the No.1 infection that leads to antibacterial drug consumption [9, 10]. Women are more affected as about 10% of females in the United States have at least one incident of symptomatic UTI each year. Almost 60% of women have one or more symptomatic UTIs during their lifespan [5].
A worldwide emerging epidemic of antimicrobial resistance is observed in varying contexts, increasing the prevalence of methicillin-resistant Staphylococcus aureus (MRSA) infection, extended-spectrum β-lactamase (ESBL)-producing organisms, and completely pan-resistant gram-negative bacilli [11-14]. Multidrug-resistant pathogens are considered a real risk to community health with a high impact on morbidity and mortality. As a result, infectious diseases still rate the second cause of global mortality despite the availability of antibiotics [15]. Our misuse of antibiotics will apply selective pressure increasing the numbers of resistant strains, particularly in developing countries [16, 17].
In Sudan, bacterial infections of the urinary tract represent a major cause of outpatient visits as well as hospital-acquired infections. The prevalence of multidrug-resistant uropathogens in Sudan is increasing, making currently used empirical therapeutic regimens suboptimal [18, 19]. An important causative factor of this is the patient’s intentional behavior of self-treatment by antibiotics [20]. Sudan, a developing country with limited resources, allocates a considerable amount of its health-payments to buy drugs, especially antibiotics. Updated knowledge of the commonest bacterial causes and their susceptibility patterns is crucial for the proper selection and use of antimicrobial drugs and the development of effective local prescribing guidelines. Moreover, they are important for the physicians in far rural areas who may not have facilities of microbiology laboratory set-up and, therefore, must rely on their knowledge of antibiotic-resistant rates. While antimicrobial resistance surges, the expenditure of treating infections will increase as more costly antimicrobial agents are needed to reach clinical and laboratory cure. Temporal and local variables can modify these policies, so they need to be constantly re-evaluated [21-23].
Unluckily, there is no available profound information on the etiology and resistance pattern of UTIs in Sudan. Many cases are observed to be resistant to conventional chemotherapy in clinical practice. Within Sudan, the majority of community-acquired UTIs are managed on an empirical basis without testing the susceptibility of detected UTI pathogens. The insufficient community-specific microbiological data stands against the ability to recommend effective first-line therapy for UTI.
2. MATERIALS AND METHODS
This is a retrospective facility-based study that was conducted in two centers in Khartoum-Sudan, the microbiology section of Elzhrawi laboratory and the microbiology section of Khartoum teaching hospital throughout seven years period (2009-2015). Elzahrawi is a referral laboratory that receives referred outpatients or inpatients from outside and within Khartoum state.
Handling of urine samples, identification of organisms, and antimicrobial susceptibility testing were made according to guidelines in Monica Cheesbrough 2000, 2006. Clean catch specimens were collected by instructing patients with suspected UTI to wash the hands, cleanse the area around the urethral opening with clean water and collect midstream urine with as little contamination as possible. 10-20 ml urine specimens were collected in sterile containers. Then the containers were labeled with the patient’s name, number and date of collection.
Urine culture was done on blood agar, Mackonkey agar or Cystine lactose electrolyte-deficient (CLED) agar using a calibrated standard loop then incubated at 35-37 °C overnight. The number of (CFU) per ml of more than 105/ml was regarded as significant bacteriuria. Identification of organisms was made by performing gram staining of suspected colonies; confirmatory identification was made using different biochemical tests. Results are interpreted as described in the guidelines mentioned in Monica Cheesbrough 2000, 2006.
Susceptibility testing was carried out by the disc diffusion method, as described in detail in Monica Cheesbrough 2000, 2006. Staphylococcus aureus ATCC 25923, Escherichia coli ATCC 25922, and Pseudomonas aeruginosa ATCC 27853 are used as control strains. A plate of Mueller Hinton agar was used for inoculation; in 30 minutes of applying the discs, aerobic incubation was performed for 16-18 hours at a temperature of 35 °C.
Due to the relatively long period of the study, different sets of antibiotic discs are used to test the susceptibility of different pathogens. Antimicrobials tested are Ampicillin 10 mcg, Cloxacillin 5 mcg, penicillin 10 Units, Ampicillin/Sulbactam 20 mcg, Methicillin 5 mcg, Cefotaxime 30 mcg, Ceftazidime 30 mcg, Ceftriaxone 30 mcg, Cefuroxime 30 mcg, Cephalexin 30 mcg, Chloramphenicol 30 mcg, Clindamycin 2 mcg, Ciprofloxacin 5 mcg, Vancomycin 30 mcg, Co-Trimoxazole 25 mcg, Gentamycin 10 mcg, Nitrofurantoin 300 mcg, Tetracycline 30 mcg, Amikacin 30 mcg, Erythromycin 15 mcg, Ofloxacin 30 mcg, Sparfloxacin 5 mcg, Doxycycline 30 mcg, Gatifloxacin 5 mcg, Imipenem 10 mcg, Norfloxacin 10 mcg, Nalidixic acid 30 mcg, Amoxicillin/clavulanic acid 30 mcg. Antibiotic discs were obtained from Axiom & HIMEDIA.
The prevalence of resistance of the pathogens against each antibiotic was calculated as the proportion of resistant isolates over the entire tested isolates. Data were analyzed using Epi info; the chi-square test was used to assess the statistical significance of results (when >20% of the cells have expected values <5, then Fisher exact test was used). Results with Probability values of <0.05 were considered statistically significant.
Ethical approval and informed consent were not needed for this study because it is a retrospective study.
3. RESULTS
In this study, 774 samples were cultured from patients with suspected UTI, 705 (91%) urinary isolates showed significant growth (>105 CFU /L) while the other 69 samples showed no significant growth. 431 (61%) of the patients were female, while the other 274(39%) were males.
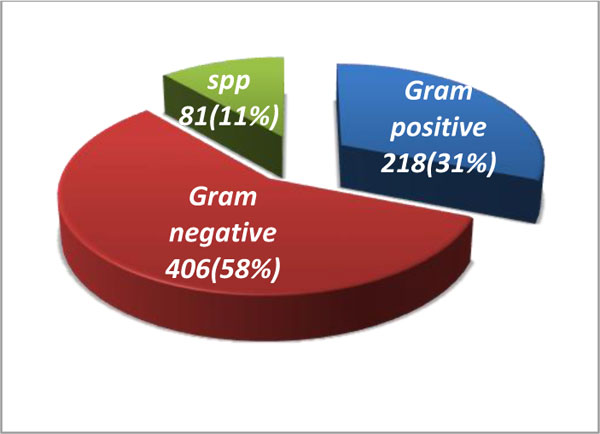
13 types of pathogens were identified in 705 urinary isolates. Gram-negative bacteria were the major isolates (Fig. 1). E.Coli was the main bacterial uropathogen followed by S.aureus, Pseudomonas, and Klebsiella (Table 1).
There was a significant difference between males and females regarding the causative organism of UTI with a P-value of 0.0087. E.coli, S.aureus & candida spp were found to cause a higher proportion of infections in females, Proteus and coagulase-negative staphylococci (CNS) were equal in both genders while the other types of pathogens were more in males (Table 2).
After the exclusion of Candida, the 624 isolates were tested for antimicrobial resistance. Microbiological susceptibility of a total of 28 antibiotics was tested; for each urinary isolate, different sets of these antibiotics were used. 601(96%) of the bacteria were resistant to at least one antibiotic. 17 antibiotics were found to have a bacterial resistance rate of more than 50%, including all B lactams except Cefurixime, Nalidixic acid, Ciprofloxacin, Norfloxacin Clindamycin, Co-Trimoxazole, and Tetracyclines (Tetracycline& Doxycycline). Other antibiotics were found to have resistance rates of less than 50%. Amikacin & Imipenem had the highest susceptibility rates. Stratified by gender, microbiological resistance to Cloxacillin, Penicillin, Ampicillin/Sulbactam, Cefuroxime, Cephalexin, Vancomycin, Erythromycin, Norfloxacin was found to be significantly higher in females compared to males (P-value<0.05). The mean of microbiological resistance to antibiotics in males was 55.08% compared to 60.54% in females.
In terms of specified treatment depending on Gram-stain morphology, our study suggests that Amikacin, Gatifloxacin & Ceftriaxone are the best parenteral antibiotics for confirmed gram-positive UTI while the best oral options were Nitrofurantoin & Ofloxacin. Gram-negative infections may be treated best with Vancomycin, Imipenem, Amikacin, Gatifloxacin & nitrofurantoin. There was a significant difference (P-value<0.05) in antimicrobial resistance of the two-gram stain morphotypes against several antibiotics (Table 3).
Imipenem was the most potent antibiotic in this study with a low rate of resistance (less than 6%), Enterococci was exceptionally resistant (60%). Ceftriaxone & Cefurexime resistance rates were variable among bacteria; S.aureus & Pseudomonas show exceptional sensitivity. Klebsiella spp & Pseudomonas were resistant to Nitrofurantoin, whereas E.coli, S.aureus, Enterococci were sensitive. Overall sensitivity to Gentamycin was high; Klebsiella & Enterococci were less sensitive. While all types of bacteria show reasonable sensitivity to Ofloxacin & Sparfloxacin, Klebsiella was highly resistant to them. Amoxicillin clavulanic acid had a low susceptibility rate except for Enterococci & Proteus (Table 4).
| Gender | S.aureus | E.Coli | Klebsiella spp | Candida spp | Enterococci | Pseudomonas spp | Proteus spp | CNS | others | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Male | 53(19) | 67(24) | 27(10) | 28(10) | 24(9) | 33(12) | 1(1) | 13(5) | 28(10) | 274 |
| Female | 85(20) | 153(35) | 33(8) | 53(12) | 29(7) | 28(6) | 6(1) | 20(5) | 24(6) | 431 |
| Total | 138(20) | 220(31) | 60(9) | 81(11) | 53(7) | 61(9) | 7(1) | 33(5) | 52(7) | 705 |
| Antibiotic | Resistance in males | Resistance in females | Total resistance | P-value |
|---|---|---|---|---|
| Ampicillin | 61(88) | 93(91) | 154(90) | 0.66 |
| Ampicillin/Sulbactam | 59(81) | 137(88) | 196(86) | 0.01 |
| penicillin | 25(71) | 30(97) | 55(83) | 0.001 |
| Cloxacillin | 12(75) | 14(82) | 26(79) | 0.01 |
| Amoxicillin/clavulanic acid | 38(79) | 60(73) | 98(75) | 0.63 |
| Methicillin | 9(60) | 18(72) | 27(67) | 0.49 |
| Cephalexin | 50(78) | 110(79) | 160(78) | 0.003 |
| Cefotaxime | 26(68) | 40(77) | 66(73) | 0.52 |
| Ceftazidime | 44(71) | 52(66) | 96(68) | 0.17 |
| Ceftriaxone | 13(50) | 27(54) | 40(53) | 0.61 |
| Cefuroxime | 1(17) | 13(57) | 14(48) | 0.04 |
| Co-Trimoxazole | 143(79) | 265(83) | 408(82) | 0.07 |
| Doxycycline | 13(81) | 15(79) | 28(80) | 0.44 |
| Tetracycline | 125(69) | 176(72) | 301(70) | 0.14 |
| Clindamycin | 67(81) | 86(72) | 153(76) | 0.12 |
| Nalidixic acid | 31(74) | 57(70) | 88(72) | 0.24 |
| Norfloxacin | 78(54) | 174(65) | 252(61) | 0.02 |
| Ciprofloxacin | 74(52) | 126(57) | 200(55) | 0.67 |
| Sparfloxacin | 22(43) | 56(47) | 77(46) | 0.11 |
| Ofloxacin | 29(36) | 60(38) | 89(37) | 0.11 |
| Gatifloxacin | 7(19) | 15(22) | 22(21) | 0.71 |
| Vancomycin | 8(40) | 10(59) | 18(49) | 0.04 |
| Erythromycin | 13(34) | 20(63) | 33(47) | 0.002 |
| Nitrofurantoin | 26(35) | 52(36) | 78(36) | 0.27 |
| Chloramphenicol | 52(38) | 70(33) | 122(35) | 0.17 |
| Gentamycin | 60(45) | 82(45) | 142(45) | 0.14 |
| Amikacin | 16(18) | 27(13) | 43(14) | 0.14 |
| Imipenem | 1(3) | 3(8) | 4(6) | 0.09 |
| Antibiotic | Resistance in GBB | Resistance in GNB | P-value |
|---|---|---|---|
| Ampicillin | 28(80) | 126(93) | 0.08 |
| Ampicillin/Sulbactam | 81(89) | 115(85) | 0.52 |
| penicillin | 35(76) | 20(100) | 0.06 |
| Cloxacillin | 14(78) | 12(80) | 0.14 |
| Amoxicillin/clavulanic acid | 24(55) | 74(86) | 0.0004 |
| Methicillin | 25(69) | 2(100) | Fisher exact 0.54 |
| Cephalexin | 64(70) | 96(86) | 0.03 |
| Cefotaxime | 26(72) | 39(74) | 0.29 |
| Ceftazidime | 21(72) | 75(67) | 0.33 |
| Ceftriaxone | 4(25) | 36(60) | 0.03 |
| Cefuroxime | 4(44) | 10(50) | 0.89 |
| Co-Trimoxazole | 128(77) | 279(85) | 0.09 |
| Doxycycline | 4(67) | 24(83) | 0.48 |
| Tetracycline | 92(63) | 207(74) | 0.02 |
| Clindamycin | 68(83) | 84(71) | 0.16 |
| Nalidixic acid | 41(80) | 47(65) | 0.15 |
| Norfloxacin | 79(56) | 172(64) | 0.03 |
| Ciprofloxacin | 64(52) | 136(57) | 0.73 |
| Sparfloxacin | 29(44) | 49(48) | 0.44 |
| Ofloxacin | 30(31) | 59(42) | 0.02 |
| Gatifloxacin | 10(20) | 12(22) | 0.77 |
| Vancomycin | 16(57) | 2(22) | 0.02 |
| Erythromycin | 23(46) | 10(50) | 0.75 |
| Nitrofurantoin | 19(28) | 59(39) | 0.04 |
| Chloramphenicol | 43(39) | 79(33) | 0.27 |
| Gentamycin | 43(47) | 99(45) | 0.91 |
| Amikacin | 21(19) | 22(12) | 0.28 |
| Imipenem | 3(60) | 1(2) | 0 |
Table 4.
| Antibiotic | S.aureus | E.Coli | Klebsiella spp | Pseudomonas | CNS | Enterococci | Proteus spp |
|---|---|---|---|---|---|---|---|
| Ampicillin | 14(74) | 65(94) | 19(100) | 6(75) | 4(80) | 13(76) | 1(100) |
| Ampicillin/Sulbactam | 63(89) | 62(83) | 28 (93) | 21(84) | 14(88) | 1(100) | 4(67) |
| penicillin | 17(74) | 10(100) | 1 (100) | 5(100) | 2(40) | 18 (90) | NT |
| Cloxacillin | 10(77) | 7(100) | 2(100) | 3(50) | 3(75) | NT | NT |
| Amoxicillin/clav | 14(70) | 46(90) | 12 (100) | 7(88) | 3(50) | 5(29) | 0 |
| Methicillin | 19 (76) | 2(100) | NT | NT | 5(45) | 1(50) | NT |
| Cephalexin | 50(68) | 52(81) | 22(88) | 17(94) | 10(71) | 1(100) | 5(100) |
| Cefotaxime | 19(73) | 16(84) | 8(62) | 10 (77) | 3(50) | 3 (100) | NT |
| Ceftazidime | 13(59) | 46(74) | 10(77) | 12(48) | 3(100) | 4 (80) | NT |
| Ceftriaxone | 2(22) | 25(60) | 5(100) | 0 | 0 | 4(50) | NT |
| Cefuroxime | 2(40) | 10(63) | 1(50) | 0 | 0 | 1(100) | NT |
| Co-Trimoxazole | 87(76) | 161(88) | 44(85) | 41 (93) | 22(79) | 17(71) | 4(67) |
| Doxycycline | 1(50) | 16(89) | 4(80) | 1(100) | 1(100) | 2(66) | NT |
| Tetracycline | 65(65) | 119(76) | 33(72) | 35(80) | 8(35) | 19(76) | 5(100) |
| Clindamycin | 47(84) | 48(73) | 12(55) | 15(83) | 7(78) | 16(89) | 0 |
| Nalidixic acid | 28(85) | 22 (67) | 6(55) | 7(100) | 1(50) | 12 (80) | 1(50) |
| Norfloxacin | 60(67) | 110(74) | 25(61) | 12 (43) | 6(29) | 16(49) | 2(28) |
| Ciprofloxacin | 49(56) | 91(65) | 24(62) | 13(33) | 7(32) | 7(58) | 0 |
| Sparfloxacin | 24(46) | 28(46) | 13(65) | 5(31) | 0 | 0 | 2(40) |
| Ofloxacin | 26(33) | 34(45) | 19(55) | 4(17) | 3(18) | 0 | 2(40) |
| Gatifloxacin | 9(22) | 5(17) | 3(23) | 3(30) | 0 | 0 | 1(50) |
| Vancomycin | 4(40) | 0 | NT | NT | NT | 14 (54) | NT |
| Erythromycin | 13(54) | 5(71) | 1(100) | 1(20) | 1(20) | 12(46) | NT |
| Nitrofurantoin | 13(26) | 18(20) | 16(67) | 12(71) | 3(38) | 1(11) | 2(40) |
| Chloramphenicol | 29(37) | 34(25) | 15(35) | 21(58) | 9(60) | 4(22) | 4(80) |
| Gentamycin | 23(45) | 53(42) | 19(68) | 8(28) | 3(17) | 21(72) | NT |
| Amikacin | 12(17) | 15(13) | 6(14) | 4(13) | 2(14) | 1(100) | 0 |
| Imipenem | 0 | 1(3) | 0 | 0 | NT | 3(60) | NT |
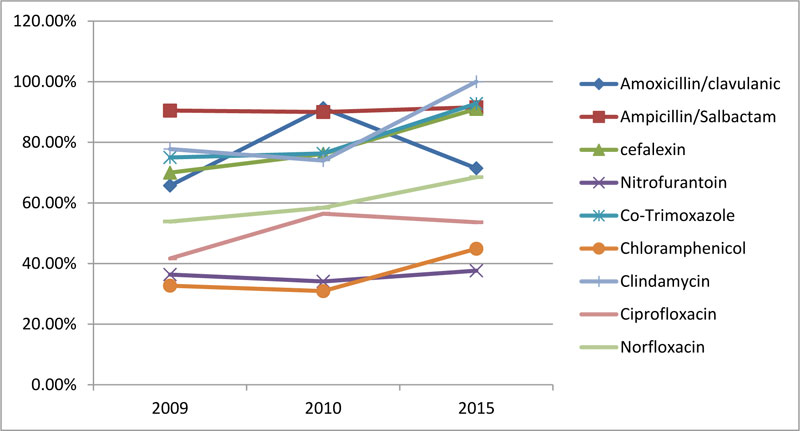
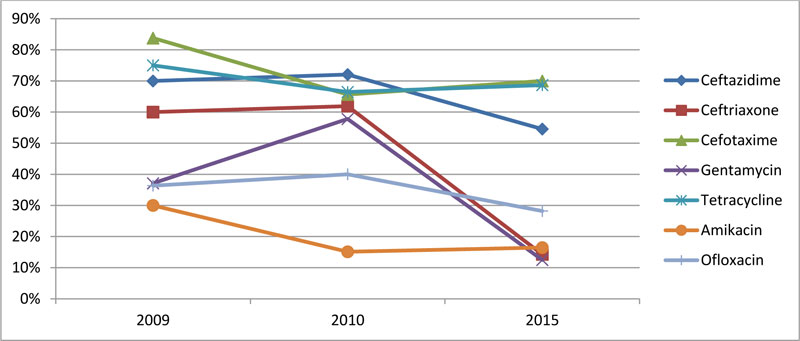
Throughout the 7 years, resistance to most of the antibiotics showed an incremental pattern. On the other hand, resistance against Aminoglycosides, Erythromycin, and 3rd generation Cephalosporins (Ceftazidime, Cefotaxime and Ceftriaxone) were significantly decreased. Tetracycline, Ofloxacin, Ampicillin & Cloxacillin resistance rates slightly decreased at the end of the study compared to the start. (Figs. 2, 3).
*Others include Salmonella typhi, Enterobacter spp., Streptococcus viridians, Difthoid spp., Citrobacter spp.
4. DISCUSSION
The high proportion of culture-positive samples seen in this study (91%) compared to previous studies may be due to urine culture being non-routine investigation in Sudan, and in most of the cases, it was done after positive indicators of infection in urine analysis [24]. Most of the samples were from female patients; this is due to the higher incidence of UTI among females because of structural differences, including the shorter urethra and the presence of physiological vaginal discharge leading to the moist periurethral area [25, 26].
Most pathogens were Gram-negative bacilli (about 60%) and E.coli is the dominant pathogenic bacteria; this finding is concordant to previous studies done in different parts of the world [24, 27-30]. Other dominant pathogens isolated in this study were Enterococcus faecalis(6.52%), Staphylococcus aureus(19.57%), Proteus spp(0.99%), Klebsiella spp(8.51%), Pseudomonas spp(8.65%), these bacteria were isolated in other study at rates of 19%, 13%, 4%, 4% and 3% respectively [31]. In addition to this study, recent studies have reported the increasing prevalence of S.aureus in UTIs [32-34].
The overall resistance rate of bacterial pathogens to antimicrobial drugs was remarkably high in this study, parallel to the results of previous studies done in Sudan [31, 35]. Multiple factors have increased the prevalence of antibiotic resistance, including the high consumption of antibiotics due to the increased incidence of infectious diseases, selective prescribing due to the effect of promotional pursuits of pharmaceutical corporations, lack of diagnostic laboratory facilities and physicians, particularly in remote areas, and the challenges in distributing data regarding antibiotic susceptibility. Another important causative factor in Sudan is the patient’s intentional behavior of self-treatment by antibiotics [20].
Heavily prescribed antibiotics and medications inappropriately used by the community like B lactams, Cotrimoxazole, Ciprofloxacin, Doxycycline were found to have high rates of bacterial resistance due to selection power on the bacterial population leading to the survival of the most resistant bacteria which have acquired methods of counteracting their mechanisms of action [36, 37]. In addition, the 7 years trend of resistance against them was incremental, indicating the problem is still in progress and ringing the bell toward putting strict strategies for an antibiotics prescription.
Various antibiotics with high susceptibility rates like Chloramphenicol & Gatifloxacin have severe side effects making the challenge of choosing drugs more difficult [38]. Besides, most of these antibiotics are available only for the parenteral route, increasing the number of hospital admission, which is in a developing country like Sudan, is far difficult and costly.
Ampicillin was the least efficacious antimicrobial agent, as only 10% of all tested isolates were sensitive to it. This finding is similar to other studies, where only 37% were sensitive to ampicillin [39]. Co-Trimoxazole (trimethoprim/sulfamethoxazole) was among the least effective drugs, and its antimicrobial resistance is increasing from about 50% in previous studies to about 82% in this study. In addition, resistance against Ciprofloxacin, Norfloxacin & Ceftriaxone was found to be higher in this study in comparison to previous surveys [24, 39]. As seen in other studies, UTI pathogens have higher resistance against amoxicillin/clavulanic acid when compared with fluoroquinolones [27].
According to their observed resistance rate in this study, Fluoroquinolones & Co-Trimoxazole should not be used as empirical treatment as the Infectious Diseases Society of America (IDSA) recommends a 10% & 20% resistance threshold for the treatment of urinary tract infections with fluoroquinolones & Co-Trimoxazole, above these rates these antimicrobial agents must not be administered for empirical therapy [40].
Although Cephalexin is commonly used in the outpatient setting for treating uncomplicated cystitis and ASB, it had a low susceptibility rate (21.5%), and as well it is not approved by the IDSA for the management of uncomplicated UTI [40].
In agreement with other studies, Imipenem & Amikacin showed the highest levels of susceptibility (94%)& (86%), respectively [39]. Susceptibility rates to Nitrofurantoin, Gentamicin, Cefuroxime remain above 50% but are decreasing from 77%, 88% & 90.1% before 2013 to 64%, 55% & 52% in this study [24, 39]. Resistance against Nitrofurantoin was relatively low (35.62%), also it is a well-tolerated oral antibiotic with a low potential for collateral damage. Therefore, it is proposed as one of the first-line antibiotics for the treatment of uncomplicated cystitis as well as chemo-prophylaxis in females with recurrent UTIs [41]. Conversely, it is not recommended the treatment of pyelonephritis because it does not achieve high concentration within the kidney’s parenchyma [42].
In agreement with a German study, gender Stratified prevalence of antimicrobial resistance was found to be generally lower among males than females [43]. The presence of this difference raises the importance of gender-stratified surveillance studies, which establish the basis of gender-specific empiric therapy.
The resistance of Klebsiella spp isolates against gentamycin in Sudan was increased from 40% in the year 2000 to 67.86% in this study [35]. In addition, resistance against 3rd generation cephalosporin and nalidixic acid was significantly increased in comparison to previous studies [31, 35, 39].
In recent years, highly antibiotic-resistant uropathogens, including ESBL producing organisms, arise as an important cause of community-acquired UTIs and healthcare-associated complicated UTIs [5]. In this study, more than 50% of isolated E.coli, klebsiella spp, coliform were resistant to all B lactams suggesting an ESBL production mechanism. Also, a study in India showed that the proportions of (ESBL)-positive isolates were 66%–77% in E. coli and 61%–72% in K. pneumoniae [44]. Based on this survey and in agreement with another study, carbapenems are the best agents to cure UTIs caused by multidrug-resistant bacteria such as ESBL producing Enterobacteriaceae [45]. According to the guidelines of the European Association of Urology, this high rate of ESBL-producing E. coli necessitate the initial therapy of pyelonephritis should be with an Aminoglycoside or Carbapenem shifted to oral antibiotics based on susceptibility testing [46]. 76% of S.aureus was resistant to Methicillin(MRSA), a result comparable to other studies on which MRSA constitutes 86% of the S. aureus isolates [47]. Unfortunately, this finding is not a local problem, it is part of an emerging global epidemic of MRSA, especially within health care institutions [48, 49].
In contrast to other isolates, Enterococci were found to be resistant to Vancomycin and Imipenem. Although Carbapenems have outstanding bactericidal action against approximately all pathogenic bacteria, Enterococci are known to be intrinsically resistant to them, especially Enterococcus faecium [50]. From 2014 onwards, the proportions of Vancomycin-resistant Enterococci(VRE) isolates increased from 11.2% in 2014 to 26.1% in 2017 [51]. In addition to enterococci, S.aurues has a resistance rate of 40% to Vancomycin; these findings put the treatment of UTI at great challenge because Imipenem and Vancomycin are one of the drugs of last resort and are used after treatment with other antibiotics have failed.
CONCLUSION AND RECOMMENDATIONS
Gram-negative organisms were the main cause of UTI. Bacteria causing UTI in Sudan frequently develop resistance against 17 antimicrobial drugs, and thus, we emphasize a serious dilemma in front of the health system. Given rising antimicrobial resistance trends, appropriate use of antibiotics and the development of novel agents are important to face this problem. To invent novel antibiotics, it is vital to study antimicrobial resistance on a molecular basis so that we can avoid and defeat mechanisms of resistance.
For all suspected cases, a culture and sensitivity test has to be conducted before the initiation of empirical antibiotics therapy and then drugs should be adapted according to the results. Personal hygiene, as prevention and hydration, may replace the use of antibiotics in many cases. Current empirical antibiotic therapy for UTI should be modified, and new guidelines should be established based on local resistance rates. This study comes up with precious regional data for evidence-based empirical antibiotic treatment, but a national sentinel surveillance system and regional antibiograms should be established to track the bacterial susceptibility profiles in Sudan. As well, antimicrobial stewardship programs are essential to provide educational activities and issue the announcement of bacterial susceptibility rates to antibiotics with the ultimate goal of appropriate and cost-effective prescription behavior.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to thank the research group for their hard and cooperative work, thanks to Elzahrawi laboratory, Khartoum teaching hospital ,to Professor Eltahir Khalil for his warmly granted helps and advices. Great acknowledgement to my family and my husband; Ammar Mandor for their support. Gratitude to the Open Microbiology Journal for their critical free advice on the manuscript.

