All published articles of this journal are available on ScienceDirect.

Comparative Study on the Use of Widal Test to Stool Culture in the Laboratory Diagnosis of Typhoid Fever in Holy Family Hospital Akum, North West Region of Cameroon
Authors Info & Affiliations
Abstract
Background:
Typhoid fever has several diagnostic tests. However, misdiagnosis is common since most health care facilities use only the Widal test without confirmation of results with a second test method.
Objective:
This study aimed at evaluating the performance of Widal test to stool culture in the Laboratory diagnosis of typhoid fever.
Methods:
Recruited in this study were 112 consented patients ≥1 year presenting with symptoms clinically suspected of typhoid fever visiting the Hospital in April, 2018. Blood and stool samples collected from all participants were subjected to Widal and stool culture, respectively. Serotyping was done using Salmonella O, and H antisera. Widal agglutination titre values ≥1:80 were considered as positive for the Salmonella antigen. Isolation of S. typhi from stool culture indicated an infection. Data was analysed using the Statistical Package for Social Sciences (SPSS). Sensitivity, specificity, Negative Predictive Value (NPV) and Positive Predictive Value (PPV) of Widal test were calculated. The sensitivity and specificity of the stool culture were 100% since it was the ideal to which the Widal test was compared.
Results:
Prevalence of typhoid fever using stool culture was 39.3%, sensitivity and specificity of Widal were 40.9% and 32.4%, respectively. NPV and PPV were 6.44% and 28.13%, respectively.
Conclusion:
Widal test is not reliable for diagnosis of typhoid fever. Health care personnel should develop a rapid, highly sensitive and cheap diagnostic method that is also capable of differentiating Salmonella infection from other infections.
1. INTRODUCTION
Typhoid fever is a communicable disease, found only in man and occurs due to systemic infection mainly by Salmonella typhi organisms [1]. It is an acute generalized infection of the reticulo-endothelial system, intestinal lymphoid tissue, and the gall bladder. Until the first quarter of the 19th century, typhoid fever was not recognized as a separate clinical disease and was often confused with other prolonged febrile syndromes such as typhus fever of rickettsial origin [1]. Typhos in Greek means smoke and typhus fever got its name from smoke that was believed to cause it. It was only late in the 19th century that the disease was finally established as a distinct clinical entity termed enteric fever [1]. Annually, 11-20 million people get sick from typhoid fever and between 128000 and 161000 people die from it [2]. In Cameroon, the prevalence of typhoid was reported in Kumba to be 7.9% [3] but this is an underestimated figure because facilities capable of performing the stool and blood culture test essential for diagnosis are absent from many regions.
Although oral contact with an infected person may result in the transmission of the bacteria, in most cases it is spread through contaminated food or water. Contaminated water and poor sanitation are the most common cause of typhoid fever in developing nations [4]. Although one can be treated with antibiotics, few who recover are still reported to harbour the bacteria for years in their gall bladder or intestinal tracts. These chronic carriers as they are referred to may infect others through shedding the bacteria in their faeces although they might not have signs or symptoms [5].
Diagnostic methods for typhoid fever currently used in health facilities in Cameroon include Widal test, stool and blood cultures. The problem, however, is the fact that in developing nations, the equipment, supplies and trained laboratory personnel required especially in primary health-care can rarely be found. Due to this, the most commonly used diagnostic method in most rural health care facilities in many countries including Cameroon is the Widal test method which is cheaper, easy to perform and does not require complicated expertise [6]. The Widal test alone is done without confirmation of results with a second test method. This at times leads to unnecessary and inappropriate antimicrobial treatment of patients without the typhoid fever due to misdiagnosis. The objective of the present study was to evaluate the performance of Widal test to stool culture in the Laboratory diagnosis of typhoid fever, with a view to review the testing algorithm for the benefit of the patient.
2. MATERIALS AND METHODS
2.1. Study Area
The study was carried out at Holy Family Hospital Akum, Santa Sub Division, Mezam Division of the North West Region of Cameroon. This area is made up of 12 quarters and has an estimated population of 5771 inhabitants whose occupation is mainly farming. The institution is situated along the Bafoussam Bamenda axis at mile 6 Akum and 17km from Bamenda town. The temperature of the area ranges from 20-21oC. Farming is their main occupation due to the fertility of the soil. They engage in cattle rearing and cultivation of crops like corn, beans, Irish potatoes, etc. The hospital is well-known for the varied health services rendered to the public. The presence of modern equipment and a high influx of patients to the hospital from all areas of North West, West, Centre and Littoral Regions on daily bases makes the institution a good centre for research.
2.2. Study Design and Period of Study
A descriptive cross-sectional study was conducted in April 2018. The study involved obtaining blood and stool samples from patients suspected of having typhoid fever. Blood samples were centrifuged to obtain serum that was subject to the Widal test. Stool samples were inoculated into BD Salmonella Shigella Agar (SSA) suitable for cultivation of Salmonella typhi.
2.3. Study Population
Participants of this study were patients clinically diagnosed as having typhoid fever and who presented with fever of 38oC and above, had bowel disturbance, headache, malaise, anorexia, etc, seeking medical attention at the Holy Family Hospital Akum. A total of 112 consented participants were enrolled in this study.
Only consented patients who presented with fever at the Holy Family Hospital Akum, aged 1 year and above were included in this study. Patients who had taken antibiotics say about a week before coming to the hospital, vaccinated individuals, those who did not present with fever and those age less than 1 year were excluded from the study.
2.4. Specimen Collection
Specimens were collected from patient > 1-year-old with symptoms of typhoid fever who presented themselves at the study site. They were asked to give verbal consent and answer brief questions about antimicrobial treatment, history of typhoid fever and vaccination. Guardians gave consent for minors. Specimens for this study were blood and stool for Widal and stool culture respectively.
5ml of blood was obtained from each study participant upon routine venepuncture for Widal test. Blood samples in plain tubes were allowed to clot and the clot removed by centrifuge and the supernatant obtained was serum.
Freshly passed faeces were collected in a sterile wide mouthed container. To avoid contamination, patients were given sterile papers to pass stool on it before picking a portion and putting in the sterile wide mouthed container. Each sample container was labelled with the patient’s code number, date and time.
2.5. Laboratory Analysis
2.5.1. Widal Slide Agglutination Test Procedure
The Swemed diagnostic Widal test kit was used to perform Widal test and was carried out in accordance to the manu-facturer’s instructions. The reagents contained Salmonella typhi O and H antigens and Salmonella paratyphi A, B and C antigens. Positive and negative controls were included and a titre greater than or equal to 1/80 indicates salmonella infection. The reagents and samples were brought to room temperature and the antigens were shaken properly to mix well before dispensing. A drop of patient’s serum to be tested was placed onto each of the required number of circles on the tile, then one drop of Widal antigen suspension was added to the reaction circles containing patient serum. Using different mixing applicator sticks provided, the tile was rocked gently back and forth and observed for agglutination macroscopically for one minute. Agglutination was a positive test result and if the positive reaction was observed with the test, it indicated the presence of clinically significant levels of the corresponding antibody in the patient’s serum.
2.5.2. Stool Culture
Faeces were inoculated onto Salmonella Shigella Agar (SSA). SSA is used for isolation, cultivation and differentiation of gram negative enteric microorganisms from both clinical and non-clinical specimens. The plates were incubated at 37oC for 24 hours. Isolation of S. typhi in stool culture indicated an infection. If there was no growth, the culture was considered negative. Presence of growth was followed by a motility test to detect the presence of motile rods. Then, a Grams stain procedure was performed to detect the presence of gram negative bacilli (rods). This was followed by a biochemical test using Kligler Iron Agar (KIA) to read acid production of the slant, gas and H2S production. The presence of a red slant, yellow butt, weak H2S reaction (black colony centres), and no gas indicated a positive KIA.
2.5.3. Data Management and Statistical Analysis
Raw data were entered into Microsoft Excel. Statistical analysis was conducted using IBM SPSS statistics 21.0. The analysis involved computation of descriptive statistics, frequencies, means and standard deviations. Statistical analysis outputs were presented in form of tables and graphs. Comparisons of categorical data were made using the Chi-square test. A P value ≤ 0.05 was considered statistically significant.
2.5.4. Ethical Consideration
Approval for this study was granted by the North West Regional Delegation of Public Health (No.687/NWR/RDPH) as well as the management of the Holy Family Hospital Akum, upon presentation of a supporting document from the School of Medical and Biomedical Sciences of National Polytechnic University Institute, alongside a research proposal. The participants were informed about the study and interested participants gave verbal consent. All records were kept confidential and only accessible to members of the immediate research team. Individuals selected for the study were identified by special code numbers. Adults gave their verbal consents to take part in the study while guardians gave verbal consents for minors.
3. RESULTS
3.1. Socio-Demographic Characteristics of Respondents
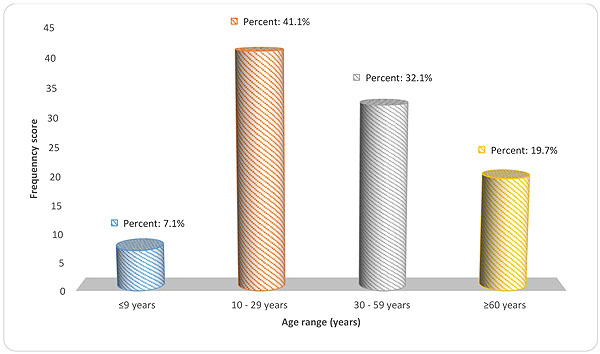
A total of 112 patients presenting with febricity at the Holy Family Hospital Akum were enrolled in this study. A majority of these respondents were females, accounting for 64.3% while 35.7% were males. With respect to age distribution, the highest percentage was accounted for by those between 10 – 29 years old (n = 46) with 41.1%. This was followed by respondents between the age range 30 – 59 years (n = 36) with a percentage score of 32.1%. Respondents from 60 years and above came next with 19.7% (n = 22) while those from 9 years and below lasted with a frequency count of 8 and percentage score of 7.1% (Fig. 1).
| Widal Test | Stool Culture | |||
|---|---|---|---|---|
| Percentage (%) | Frequency Score | Percentage (%) | Frequency Score | |
| Positive | 57.1 | 64 | 39.3 | 44 |
| Negative | 42.9 | 48 | 60.7 | 68 |
| Total | 100.0 | 112 | 100.0 | 112 |
3.2. Prevalence of Typhoid Fever with Widal and Stool Culture Tests
Out of the 112 participants in this study, 64 were positive for typhoid fever based on the Widal test with an antibody titre of 1:80 for both “O” and “H” antigens being taken as cut off point values indicative of a recent typhoid infection giving a prevalence of 57.1%. 42.9% (n = 48) on the other hand were negative for typhoid fever when used Widal as the diagnostic tool. Interestingly, the prevalence of typhoid fever was 39.3% (n = 44) based on the findings from stool culture. A total of 60.7% were proven negative for typhoid fever (n = 68) based on the same findings from stool culture and still from the same sample under study (Table 1).
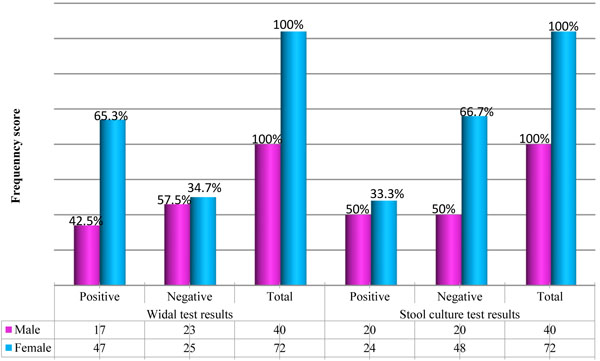
At 0.05 significance level, there was a statistically significant relationship between gender and Widal test outcomes within the study population (X2 = 5.448, P = 0.020, df = 1). With respect to the Widal positive outcome, females dominated with 73.44% while males came with 26.56%, interval of 23.21 – 36.54 (OR = 0.393) (Fig. 2).
The same scenario was observed with stool culture results when compared between the gender variable. Females came highest with 54.55% as compared to males with 45.45%. With stool culture, females were 0.531 times more liable to be positive than males, despite the fact that there was no statistical significance between gender and stool at 95% confidence interval (X2 = 2.995. P = 0.107, df = 1, CI = 28.35 – 39.95) (Fig. 2).
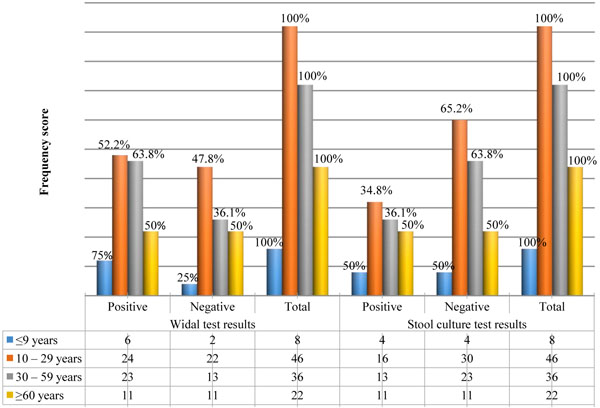
There was no statistical significance between age range within the respondents and Widal test outcome (X2 = 2.633, P = 0.452). Respondents within the age range of 10 – 29 years dominated with Widal positive results with a percentage score of 37.50%. The least came from respondents with 9 years and below with a percentage score of 9.38% (Fig. 3).
| - | Salmonella colonies | Total | |||
|---|---|---|---|---|---|
| WIDAL Test | - | - | Present | Not present | - |
| Positive | Count | 18 | 46 | 64 | |
| % within salmonella colonies | 40.9% | 67.6% | 57.1% | ||
| Negative | Count | 26 | 22 | 48 | |
| % within salmonella colonies | 59.1% | 32.4% | 42.9% | ||
| Total | Count | 44 | 68 | 112 | |
| % within salmonella colonies | 100.0% | 100.0% | 100.0% | ||
| Variable | Characteristic | Frequency | Percentage (%) |
|---|---|---|---|
| Salmonella colonies | Present | 44 | 39.3 |
| Not present | 68 | 60.7 | |
| Total | 112 | 100.0 | |
| Gram reaction | Negative rods | 44 | 39.3 |
| NA | 68 | 60.7 | |
| Total | 112 | 100.0 | |
| Motility | Motile | 44 | 39.3 |
| NA | 68 | 60.7 | |
| Total | 112 | 100.0 | |
| KIA | *Positive | 44 | 39.3 |
| NA | 68 | 60.7 | |
| Total | 112 | 100.0 |
The same thing was observed in stool culture where respondents from 10 – 29 years old dominated with 36.36% while those 9 years and below lasted with 5.88% (X2 = 1.987, P = 0.575) (Fig. 3).
3.3. Sensitivity and Specificity of Widal and Stool Culture Tests to Diagnose Typhoid Fever
The sensitivity, specificity, negative and positive predictive values were computed for Widal test compared to the stool culture technique in the diagnosis of Salmonella species. Stool culture-confirmed typhoid cases were regarded as the “true positives” and all other febrile patients with stool culture outcomes as negative for S. typhi were also considered as the “true negatives” in this study. This means that since stool culture was considered the ideal to which Widal would be compared to, its sensitivity and specificity when cultured for S. typhi using the SSA were 100% each.
Widal sensitivity was 40.9% while its specificity was 32.4% as compared to the ideal 100% sensitivity and specificity of stool culture using the SSA (Table 2). The Positive Predictive Value (PPV) and Negative Predictive Value (NPV) of Widal were 28.13% and 6.44% respectively.
3.4. Reliability, Promptness and Accuracy of Widal to Stool Culture in the Diagnosis of Typhoid Fever
A total of 44 colonies on SSA were identified, all of which were further confirmed as motile Gram-negative rods. This accounted for 39.3% positive motility test, confirmed with the same 39.3% positivity in the KIA test (Table 3).
4. DISCUSSION
4.1. Prevalence of Typhoid Fever
The findings in the present study suggest a high prevalence of 39.3% in patients using the stool culture method and a prevalence of 57.1% using the Widal test method. These high results concur with the study carried out by Gemechu and colleagues, which showed a high prevalence of typhoid fever (20%) using stool culture and 68.4% using Widal test method [7]. The high Widal prevalence in the present study could be associated with cross-reacting antibodies from febrile patients other than typhoid fever. In addition, the high prevalence of bacteria in the stool culture could be due to overcrowding with poor access to clean water and sanitation. Faecal matter may gain access into the water through runoff water or through sewage from sewers and pit latrines. This could have been a major contributing factor to the high prevalence considering that a number of patients use bushes to dispose of their faecal waste and urine.
Results from this study also showed that people of all ages are susceptible to infection by S. typhi. The age group more susceptible to the present study was those between 10-29 years old. These results concur with the study carried out by Ramyil and colleagues which showed that those between 24-29 years were more susceptible to typhoid fever [8]. This could be due to improper sanitation and hygiene. Both children and adults can get typhoid fever through ingestion of contaminated food and water. Travelling to high-risk destinations presents a high risk of contracting typhoid fever [9]. People living in overcrowded areas with poor access to safe drinking water and proper sanitation facilities are prone to infection by typhoid fever. Unlike in the present study where age was not significantly associated with S. typhi infection, a study by Lunguya and colleagues found that older age and longer duration of fever were predictive of typhoid fever [10].
A statistical significant relationship was found between gender and Widal test outcomes. With respect to the Widal positive outcomes, females dominated males meaning using the Widal test, females are more likely to be positive as compared to males. The same scenario was observed with stool culture results as females showed more positive than males. These findings contradict with the study carried by Youssef and colleagues which showed that the attack rates by S. typhi are similar for both men and women [11]. These findings also contradict with those of a study carried out by Ramyil and colleagues which showed that the males were more positive to Widal test and stool culture than females [8]. Some of the reasons why the present study showed more attack rates of S. typhi infection in females could be because women in this area are more involved in outdoor activities exposing them to high risk of infection.
4.2. Sensitivity, Specificity, Positive Predictive Value and Negative Predictive Value of Widal Test
Results demonstrated that Widal test had a low sensitivity and specificity of 40.9% and 32.4% respectively. These findings contrast with those of a study by Gemechu and colleagues which showed that Widal test had a high sensitivity of 84.2% and specificity of 35.5% [7]. False positives in the present study are possibly because the O and H agglutination usually appear around 8-12 days of infection. Hence, the probability of them not being detected during early diagnosis, and in immunosuppressed patients since they lack antibody responses. In the present study, a single sample test was used, as is the case in hospitals since outpatients rarely return for medical follow-up. This could be a drawback to interpreting the results, because of high background rates of circulating antibodies to S. typhi. Due to polyvalent nature of Widal antigens, there is a high possibility of cross-reactivity with bacterial and non-bacterial infections. Since some diseases such as malaria, ulcerative colitis, non-typhoidal Salmonella, rheumatoid arthritis and nephritic syndrome may show similar symptoms and produce high “O” antibody test, they should always be evaluated as differential diagnosis [12]. The base titre value of 1:80 may change in the population. So, the titre values may not have had much significance. The accurate antibody levels of individuals (Steady-state base lines titre) are difficult to establish. The case of many false positive in Widal test in the present study could be because individuals who had S. typhi infection in the past may have developed S. typhi antibodies during an unrelated or closely related infection, thereby giving false results.
The PPV and NPV of Widal test were low that is, 28.13% and 6.44% respectively. This means that out of the 57.1% reported cases of positive Widal in this study, the probability that subjects screened as positive truly had the disease was 0.28. The probability that subjects screened as negative using the Widal test truly were negative was 0.635. This contrast with that from a study carried out by Gemechu and colleagues which showed PPV and NPV of 24.6% and 90.0% respectively [7]. Though the PPV and NPV in this study were low, it indicates that Widal test was a slightly more better test to rule in the presence of the disease and a very poor method to rule out the presence of the disease.
Stool culture in the present study was considered the ideal to which Widal would be compared. Its sensitivity and specificity when cultured for S. typhi using the SSA were 100%. S. typhi is an enteric microorganism and its principal habitat is in the intestine of humans, so it is easily detectable in stool even in cases of early ingestion of bacteria [13]. Stool culture is important for diagnosis since it may be positive even when blood culture is negative and it is also important for the monitoring of carriage of S. typhi after apparent clinical cure, which is a risk factor for people involved.
In the present study, females were more susceptible to S. typhi infection than males which contrast findings in a study by Prajapati and colleagues where higher proportions of infection were observed in males than in females in Nepal [13]. The difference could be attributed to the fact that the study population in Nepal were children and outdoor activities more pronounced in males than in females in that area.
4.3. Reliability, Promptness and Accuracy of Widal Test to Stool Culture in the Diagnosis of Typhoid Fever
Stool culture was taken as an ideal test to which Widal would be compared. Stool culture is reliable, prompt and accurate since the 39.3% positive motility test was confirmed with the same 39.3% positivity in the KIA test whereas Widal test showed false positive and false negative results.
CONCLUSION
The prevalence of stool culture and Widal test methods was 39.3% and 57.1%, respectively. The study established that the Widal test has low sensitivity (40.9%), specificity (32.4%), NPV (6.44%) and PPV (28.13%). Widal test is not very reliable, prompt and accurate for the diagnosis of typhoid fever since false positive and negative results were common. Health care personnel should not totally depend on the Widal test alone for the diagnosis of typhoid fever but should use other diagnostic methods to differentiate Salmonella infection from other infections. Sensitisation on the modes of transmission, need for proper hygiene and sanitation should be emphasized. There is a need to develop a rapid, highly sensitive and cheap diagnostic tool for diagnosis of typhoid fever.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Approval for this study was granted by the North West Regional Delegation of Public Health (No687/NWR/RDPH) as well as the management of the Holy Family Hospital Akum, upon presentation of a supporting document from the School of Medical and Biomedical Sciences of National Polytechnic University Institute, alongside a research proposal.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
All records were kept confidential and only accessible to members of the immediate research team. Individuals selected for the study were identified by special code numbers. Adults gave their verbal consents to take part in the study while guardians gave verbal consents for minors.
AUTHOR'S CONTRIBUTIONS
CNA and ECW designed the study. CNA, ECW, and LAA performed sample collection and laboratory analyses. ANW and LFS performed statistical analyses. All authors participated in the write-up and approved the final version of the manuscript.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Sincere appreciations to the participants of this study who dedicated their time to provide us with blood and stool samples for this study. Special thanks to the staff of Holy Family Hospital Akum for the serene atmosphere and collaboration they granted us which eased the realisation of this work.

