All published articles of this journal are available on ScienceDirect.

Respiratory Tularemia: Francisella Tularensis and Microarray Probe Designing
Abstract
Background:
Francisella tularensis (F. tularensis) is the etiological microorganism for tularemia. There are different forms of tularemia such as respiratory tularemia. Respiratory tularemia is the most severe form of tularemia with a high rate of mortality; if not treated. Therefore, traditional microbiological tools and Polymerase Chain Reaction (PCR) are not useful for a rapid, reliable, accurate, sensitive and specific diagnosis. But, DNA microarray technology does. DNA microarray technology needs to appropriate microarray probe designing.
Objective:
The main goal of this original article was to design suitable long oligo microarray probes for detection and identification of F. tularensis.
Method:
For performing this research, the complete genomes of F. tularensis subsp. tularensis FSC198, F. tularensis subsp. holarctica LVS, F. tularensis subsp. mediasiatica, F. tularensis subsp. novicida (F. novicida U112), and F. philomiragia subsp. philomiragia ATCC 25017 were studied via NCBI BLAST tool, GView and PanSeq Servers and finally the microarray probes were produced and processed via AlleleID 7.7 software and Oligoanalyzer tool, respectively.
Results:
In this in silico investigation, a number of long oligo microarray probes were designed for detecting and identifying F. tularensis. Among these probes, 15 probes were recognized as the best candidates for microarray chip designing.
Conclusion:
Calibrated microarray probes reduce the biasis of DNA microarray technology as an advanced, rapid, accurate and cost-effective molecular diagnostic tool with high specificity and sensitivity. Professional microarray probe designing provides us with much more facility and flexibility regarding preparation of a microarray diagnostic chip.
INTRODUCTION
Francisella as the single member of Francisellaceae family has no intimate phylogenetic relatives to other pathogenic bacteria. There are just some far phylogenetic relationships between Francisella, Legionella, and Coxiella burnetti [1, 2].
There are four well-known subspecies belonging to Francisella tularensis (F. tularensis) including holarctica (Type B), mediasiatica, novicida, and tularensis (Type A). F. tularensis subsp. tularensis is recognized as the most deathful subspecies which encompasses a vast range of virulent factors [3-5].
The intracellular gram negative bacterium of F. tularensis is an invasive pathogenic microorganism which may lead to fatal infectious disease of tularemia in the host with a low infective cell number of 10. The zoonotic infection of tularemia is clinically divided into six forms of Glandular, Oculoglandular, Oropharyngeal, Respiratry, Typhoidal and Ulceroglandular diseases [5-10].
Respiratory tularemia is recognized as the most severe form of tularemia with a mortality rate up to 30% if not treated; therefore, F. tularensis is known as a potential biological weapon and categorized in group A of bacterial pathogenic agents [1, 7, 11-15].
Because of the life threatening and severity of respiratory tularemia, the use of a rapid, accurate, and reliable diagnostic technique is an urgent. An accurate diagnosis may lead to a definite and effective treatment. Hence, among different diagnostic methods such as microbiological cultures, serological assays, Polymerase Chain Reactions (PCRs) including real-time PCR, Enterobacterial Repetitive Intergenic Consensus PCR (ERIC-PCR) etc. and other routine techniques, the advanced molecular technique of DNA microarray is recommended [16-22].
DNA microarray technology is an advanced pan-genomic diagnostic technique which is consisted of two main parts including Dry Lab and Wet Lab. The bioinformatic section which covers the dry lab procedures is known as the in silico portion of the DNA Microarray technique. So, the probe designing processes construct the dry lab section of the tool. The wet lab of the technique concludes the in vitro portion of the technique. The wet lab section is composed of probe printing on a suitable coated surface of a glass slide (by robotic spotter), labeling of target bacterial genome (by fluorescent dyes such as Cy3 and Cy5), hybridization process (manually or automatically) and scanning. Even an ideal performed wet lab section is completely depended on the accuracy of probe designing procedures. An appropriate microarray probe designing guarantees the accuracy of outcomes resulted from DNA microarray technology and reduces the probable biases. Of course, a non-expertized done probe designing predominates the expertized wet lab procedures and gives huge noises, biases and enormous errors in final data. A well done microarray probe designing guarantees a rapid, accurate, sensitive, specific and cost effective diagnostic technique when the number of clinical specimens is high [16, 19, 20, 23-28].
Therefore, the main goal of the present research is to provide and design best candidates of microarray probes for diagnosing F. tularensis.
MATERIAL AND METHODS
As mentioned before, F. tularensis involves four subspecies of holarctica (Type B), mediasiatica, novicida, and tularensis (Type A). Besides, F. philomiragia is another species within the genus. However, there are considerable similarities between species and subspecies [1, 2, 29-31].
For this reason, the authors have used GView Server (https://server.gview.ca) to show unique sequences in F. tularensis subspecies and F.philomiragia (Fig. 1) [24, 25, 32, 33].
Regarding to GView Server application, the “unique genome” was selected for analysis type. Then the .gbk file belonging to F. tularensis subsp. tularensis FSC198 chromosome complete genome was downloaded from NCBI FTP site in FASTA format (http://ftp.ncbi.nlm.nih.gov/genomes/Bacteria/), zipped and uploaded as a reference genome [24, 25, 32-34].
Then, the downloaded .fna files belonging to F. tularensis subsp. holarctica LVS (Type B), F. tularensis subsp. mediasiatica, F. tularensis subsp. novicida (F. novicida U112), and F. philomiragia subsp. philomiragia ATCC 25017 from (https://lfz.corefacility.ca/panseq/analyses/) were also zipped and uploaded for comparing their genomes with the genome of F. tularensis subsp. tularensis FSC198 (Fig. 1). All of the parameters in GView Server were set up as default position of the server [24, 25, 32, 34, 35].
For determining and analysing the unique sequences of F. tularensis subsp. tularensis FSC198 (NC_008245), the PanSeq Server (http://blast.ncbi.nlm.nih.gov/Blast.cgi?PROGRAM=blastn&PAGE_TYPE=BlastSearch&LINK_LOC =blasthome) was used. To perform the analysis throughout the novel region detector, F. tularensis subsp. tularensis FSC198 (NC_008245) presumed as the selected query and the other aforementioned species and subspecies were determined as selected references. Because of high genomic similarities among F. tularensis subspecies, the F. tularensis subsp. tularensis FSC198 complete genome was compared only with F. philomiragia subsp. philomiragia ATCC 25017 chromosome complete genome. The related parameters in PanSeq Server were set up according to default choices [1, 2, 24, 25, 29-31, 33].
The unique sequences of F. tularensis subsp. tularensis FSC198 were finally detected and blasted by the BLAST tool which is accessible via NCBI (http://blast.ncbi.nlm.nih.gov/Blast.cgi? PROGRAM=blastn & PAGE_TYPE= BlastSearch& LINK_LOC=blasthome) [16, 19, 24, 25, 33, 34, 36, 37].
The super unique regions identified by BLAST tool were then processed for microarray probe designing. Therefore, the AlleleID 7.7 software was used for designing long oligo microarray probes. The length of probes were selected between 55 and 64 nucleotides. Other parameters regarding AlleleID software were selected in accordance with default forms [16, 24, 25, 33, 34].
The designed probes were then evaluated via NCBI BLAST tool. The confirmed microarray probes were finally tested by oligoanalyzer 3.1 (https://eu.idtdna.com/calc/analyzer) (an online tool) for appropriate structure and suitable physico-chemical characteristics. The related properties were identified via hairpin button. Other parameters were presumed as default position. Finally, the proper microarray probes were designed and produced to prepare a diagnostic DNA microarray chip [16, 19, 24, 33, 34, 36].
RESULTS
The genomic maps relating to each species and subspecies are shown in Fig. (1). The figure indicates the comparative pangenomic result obtained from pangenome analysis achieved by GView Server. Each color is pertaining to an individual strain. The colored regions involved similar sequences relating to genomes while the white regions are unique sectors among bacterial cases.
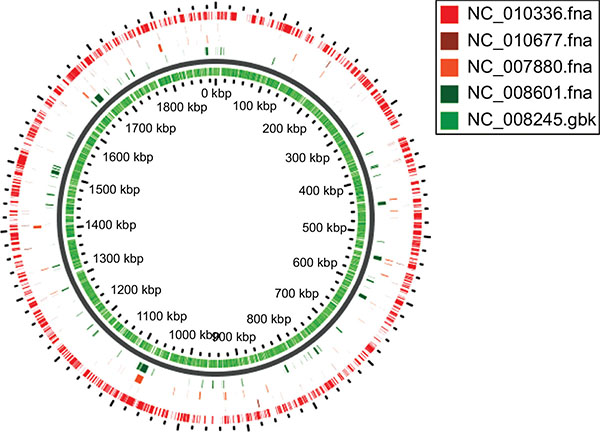
In addition to Gview server, the pan-genomic analyses achieved by PanSeq server. The results revealed unique genomic sectors within the aforementioned species and subspecies genomes including F. tularensis subsp. tularensis FSC198 (NC_008245), F. tularensis subsp. holarctica (NC_007880), F. tularensis subsp. mediasiatica (NC_010677), F. tularensis subsp. novicida (F. novicida U112) (NC_008601), and F. philomiragia (NC_010336). These analyses were vital for recognizing the unique regions for each strain.
The utilization of important pangenomic servers like Geview and PanSeq, BLAST tool (NCBI), probe designing soft ware of AlleleID 7.7 was necessary for obtaining 15 probes as the best candidate long oligo DNA microarray probes for detection and identification of F. tularensis. The processed and best candidate long oligo DNA microarray probes with high sensitivity and specificity are indicated in Table 1. These suggested probes were appropriate for recognition of F. tularensis [24].
| Microorganism | Long oligo Microarray Probe | Length | Location and gene product |
|---|---|---|---|
| F. tularensis | ATATTCTACTAAAGTCCTACTTCCATCAGCAGGGCACAATTCTTGACCATCAGGTAA | 57 |
115132-115188 Hypothetical protein |
| ACGTTACCTGACAATATAGACAGTGACAAAATAGAAGCTAAATACAGTAATGGTGTACTAAGC | 63 | 118942-119004 molecular chaperone Hsp20 | |
| TGTGCTTACAAGGGAAAGGCTATGCTTTATTACCAAAGTCAGACATTATAGACGAAA | 57 |
1861738-1861794 Hypothetical protein |
|
| AGAGACATCGTAATTAATAAACATGAAGAAGGTATGACGGAGTTCGAGCTGAGTAAGTTT | 60 |
3776-3835 Transposase family protein |
|
| AGGGACTTCGATTATATAGTTACCATTGATGTAATATACTGTACCTCCAGCAACAACTGC | 60 |
10755-10814 Membrane protein |
|
| CGTCGAAATTACATCAATAGTCGCATTTATCTTAACAGTTCTTATATATCGTGAGCATTGGCT | 63 |
16750-16812 Nicotinamide mononucleotide transporter |
|
| AGAGTCAGGAGAGATTGAGCCAATATCTTTGCCACTTATACTAATTGTGTAGTTAATAGC | 60 |
20655-20714 Chitinase |
|
| TAGATAATGTGCTTTGGTCAGGTCGGGTTGCTGATAAATCAAATAACGAGGTAAACA | 57 |
18798-18854 SAM-dependent methyltransferase |
|
| AAGTTAGATGCTTTAGTATTTACAGGAGGTATTGGTGAGAATGCTGCTAATATCCGT | 57 |
96305-96361 Acetate kinase |
|
| TACTACTTGGCTGGATCGGTGTTCGCTTGATGAATAAATCAGATGATGGTAATACTCT | 57 |
1859056-1859113 Sodium:proton antiporter |
|
| AACATCAGTATCTAATCCACTACCTCGAATCTTACACAAAGCAACATCTATCCCATCT | 58 |
29176-29233 Anhydro-N-acetylmuramic acid kinase |
|
| AGAACCTCTTAGTCGTATTTACTATTACTTAGCCGTGCCAATTACCAGCAAATCAGTTAAAGA | 63 |
38292-38354 Hypothetical protein |
|
| ACAACCATCACCATCCTTATCCGATGTAACTACAAGTTCATGTCCTAGTTCTTCTAA | 57 |
1873414-1873470 Formate dehydrogenase |
|
| TTTCATAATAACACCATTTATCGCAGCACCAACAACAAACCCAGCAATAAGTATCGC | 57 |
51911-51967 Membrane protein |
|
| TAACACTAGAACCATGCTGTCACTGTGGAAGAACTCCTCCCTGTACTGATACCATAAT | 58 |
33959-34016 Pyrimidine reductase |
DISCUSSION
Tularemia is recognized as a reemerging infectious disease with a high number of outbreaks in different countries. Besides, there are many similarities between respiratory tularemia and other respiratory infectious diseases such as mycobacterial tuberculosis, mycotic and different bacterial pneumonia, lung abscess, lung lymphoma, lung carcinoma, influenza and acute respiratory distress syndrome (ARDS). The general clinical demonstrations relating to pulmonary tularemia are variable from bronchitis, bronchopneumonia and pharyngitis to hilar lymphadenitis and pleuropneumonitis [6, 13, 15, 38, 39].
Because of the severity of respiratory tularemia and its fast progression within the host tissues, a rapid, accurate, sensitive, specific, reliable and cost effective diagnostic technique like microarray technology is needed for an appropriate diagnosis and a definite antibiotic therapy [8, 16-20, 23, 40-44].
There are different traditional microbiological diagnostic methods including direct microscopic observations of clinical specimens, histological studies, medium culture, serological assays, enzyme linked immuno sorbent assay (ELISA), and imaging. But these techniques are time consuming with low specificity and sensitivity [6, 7, 45].
PCRs such as nested PCR, ERIC PCR, real-time PCR are suitable diagnostic assays with high accuracy, sensitivity and specificity when the number of samples is low. They also are cost effective; but, they are not accurate, sensitive, specific and cost effective in the cases with huge number of specimens [16, 17, 21, 24, 25, 36, 41, 43, 46].
Indeed, the microarray technology is used for detection and identification of several microbial DNA sequence targets which are mixed within a clinical specimen [22, 47].
The microbial genomics has increased the optimization of diagnostic methods during last decade. The progression of free web databases and next generation sequencing (NGS) technologies such as DNA microarray provide us with a rapid, and reliable diagnostic tool for accurate detection and identification of pathogenic agents in microbiological samples to have definite therapeutic methods [16, 19, 20, 41].
Despite the importance of each procedure of DNA microarray technique, the probe designing performance is a critical and considerable procedure which makes DNA microarray technology a rapid, reiable, accurate, sensitive, specific and flexible diagnostic method. The sequence, calibration and the length of microarray probes directly affect the quality of analytical outcomes [16, 23-25, 33, 42, 48].
DNA microarray technology is an advanced diagnostic tool which enables us to detect and identify the target DNA sequences among hundreds of thousand sequences, genes, and microorganisms. As, the human respiratory tract possesses a complicated microbiome and the pathogenic agents of this tract include bacteria, fungi, parasites and viruses, so DNA microarray technology is a proper and preferred diagnostic tool [16, 20, 43, 49, 50].
According to the text above, rapidity and accuracy are two important factors in association with recognition of respiratory tularemia; Because, a rapid and accurate diagnosis may lead to a fast and definite treatment which resulting in improvement and reducing the mortality rate among patients with pulmonary tularemia. Moreover, the possibility of microarray probe designing provides us to have a vast range of probes. This ability makes DNA microarray a flexible, easy, simple, cost effective and useful technique. Moreover, the DNA microarray technique is able to recognize multi-drug resistant microbial strains [24, 26, 33].
CONCLUSION
Microarray probe designing enables us to choose the best candidates among several choices and to design a microarray chip with local genomic microbial species and strains with high efficacy. An expert of microarray probe designing, reduces the cost of chip upgrading process.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
This research was supported by a grant provided by Deputy of Research and Technology, Ministry of Health and Medical education, Tehran, Iran.

