All published articles of this journal are available on ScienceDirect.

Diagnosis of Respiratory Syncytial Virus Infection
Abstract
Respiratory syncytial virus (RSV) is one of the most important pathogen causing severe lower respiratory tract infections in all age groups often requiring hospitalization. Rapid laboratory diagnosis of RSV infection significantly decreases the use of antibiotics, additional laboratory testing and is associated with shorter hospitalization periods. The specific diagnosis of RSV infection is based on the detection of virus or viral antigens or virus specific nucleic acid sequences in respiratory secretions. The kind and quality of the clinical specimen exerts a considerable influence on the results of all currently used viral detection assays. Antigen based tests are widely available, easy to perform and the results are available in a short time but their reduced sensitivity and specificity represent a considerable shortcoming. Among the methods available isolation in cell culture was considered the gold standard for the sensitive identification of RSV but is gradually replaced by highly sensitive and specific nucleic acid amplification assays that provide more rapid results. Of these reverse transcription polymerase chain reaction (PCR) was the first and is still the most frequently used nucleic acid-based assay. New methodologies, as for example the real-time PCR methods allow the quantification of viral nucleic acids in the clinical sample. Disadvantages of the nucleic acid based assays are their high costs and their limited standardization.
Future research on new methodologies for the diagnosis of viral respiratory tract infections should focus on the development of sensitive, rapid and cost effective test systems allowing the screening for all probable causative agents. In addition varying testing protocols for summer and winter months based on epidemiologic data are needed to direct their practical use.
INTRODUCTION
Respiratory syncytial virus (RSV) is one of the most important respiratory pathogens, causing severe infections of the lower respiratory tract in infants, small children, the elderly, and in immunosuppressed patients, often requiring hospitalization [1-7]. RSV is highly contagious and gives rise to yearly epidemic outbreaks of respiratory tract infections during the late fall, winter and early spring with only sporadic cases detected year round [1, 8-10] (Fig. 1).
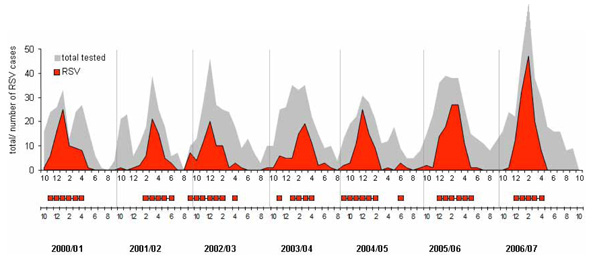
Seasonality of respiratory syncytial virus (RSV) in Austria from 2000 to 2007 (top panel). The weeks of onset and offset of RSV activity (bottom panel) are defined as the first of two consecutive cases when > 10% of respiratory secretions test positive by PCR and the last week of > 10% positive tests preceding 2 consecutive weeks of < 10% positive tests, as described in the annual report NREVSS 2005 [11].
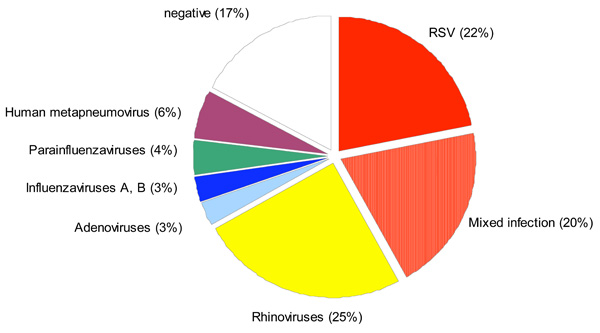
Detection of respiratory viruses in NPAs obtained from 772 infants hospitalized with acute respiratory tract illness from October 2000 through July 2004 [17].
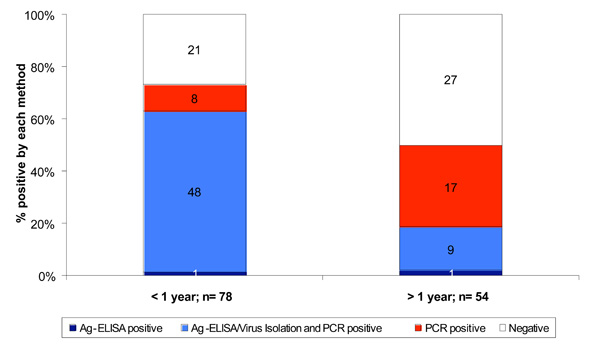
Detection of Respiratory Syncytial Virus in NPAs by semi-nested RT-PCR, Ag-ELISA and Virus isolation with regard to the patient’s age [70].
Almost all children have serologic evidence of RSV infection by 2 years of age. Primary RSV infection is rarely asymptomatic and the peak period of serious illness due to RSV is during the first few months of life with average annual hospitalization rates of 17 per 1000 children under 6 months of age and 3 per 1000 children under 5 years of age [12]. Underlying conditions, most frequently premature birth or cardiopulmonary disease are additional risk factors for severe RSV disease requiring hospitalization [13, 14]. In addition, previous RSV infections do not confer protection and reinfections throughout life are very common [15, 16]. Despite an increasing number of newly identified respiratory viruses, RSV remains the most important etiologic agent in infants below two years of age hospitalized with acute respiratory tract infection (Fig. 2).
Due to the high number of potential pathogens that may cause similar symptoms of respiratory illness, clinical characteristics are rarely distinctive enough to accurately discriminate RSV-related from other, non-RSV-related respiratory tract infections [18, 19]. Laboratory confirmation of clinically suspected RSV infection generally depends on the detection of the virus in respiratory secretions of the patient. Immunofluorescent staining of viral antigens in respiratory epithelial cells, introduced by Philipp Gardner in the 1970ies [20, 21] was the first specific rapid diagnostic test. Since then rapid, sensitive and specific diagnostic tools have been developed and their increasing availability and use unveiled the prominent role of RSV in lower respiratory tract infection in childhood and the strong association of RSV bronchiolitis in infancy and wheezing in later childhood [22-24]. The following article will provide a short review on the diagnostic value, the advantages and limitations of the most currently used techniques for RSV diagnosis.
Clinical Manifestations
RSV infection is associated with a variety of clinical manifestations ranging from mild cold-like symptoms to severe lower respiratory tract illness with significant wheezing, breathing difficulty, cyanosis and possibly apnoeic episodes. Between 25% and 40% of children develop symptoms of bronchiolitis or pneumonia during their primary RSV infection [25-28]. In addition to the more common symptoms of lower respiratory tract infection a variety of extrapulmonary manifestations, ranging from cardiac involvement to sepsis-like syndrome have been observed in children with severe RSV disease [29, 30], but whether they represent direct or indirect effects of the virus is unclear. In premature infants RSV infection is frequently atypical in its clinical presentation and may manifest as apnoea, bradycardia, or changes in feeding and ventilation [13, 31].
Reasons for RSV Testing
Rapid laboratory confirmation of RSV infection results in a reduced number of ancillary tests, a decrease in antibiotic use and shorter hospitalization periods in clinical paediatric practice [32, 33]. Laboratory diagnosis is also required for children with atypical clinical presentations, such as respiratory distress or sepsis like syndrome and in premature infants with non-specific signs in order to rule out another cause and to avoid delayed diagnosis. As RSV is highly contagious, rapid identification of RSV infected infants in hospital wards is of utmost importance in order to initiate appropriate infection control precautions to prevent nosocomial outbreaks [4, 13, 34]. Viral testing using rapid and sensitive assays for the detection of RSV are also required to take the offensive for preventive programs and to assess the efficacy of antiviral prophylaxis [35, 36]. Other reasons for viral testing exist, such as for research and epidemiologic monitoring of RSV activity.
Laboratory Diagnosis
The specific diagnosis of RSV infection is made by the detection of the virus or viral antigens or virus specific nucleic acid sequences in respiratory secretions. The kind and quality of the clinical specimen exerts a considerable influence on the sensitivity and specificity of all viral detection assays currently available. It has been demonstrated that a nasal wash or a nasopharyngeal aspirate is more sensitive for the detection of RSV than a nasopharyngeal swab specimen [37, 38]. However the collection of a nasopharyngeal swab is far less unpleasant for the patient, does not require specialized equipment, and can also be performed in an out-patient setting. Using the recently designed flocked-nasopharyngeal-swabs, which effectively dislodge and collect virus infected cells lining the nasopharynx greatly improves the quality of swab specimens and significantly increases the diagnostic yield of this clinical specimen [39-42].
Laboratory methods currently available for the detection of RSV include virus isolation in tissue culture, detection of viral antigens by direct or indirect immunofluorescent (IF) staining (DFA/IFA) or by enzyme-linked immunosorbent assays (EIAs) and the detection of viral nucleic acids by amplification assays, predominantly reverse transcription polymerase chain reaction (RT-PCR).
Virus Isolation in Tissue Culture
Isolation of RSV in tissue culture was considered as the gold standard for confirmation of presumed RSV infection for quite a long period of time. However besides the technical expertise in appropriate specimen handling for efficient virus recovery, this technique requires an average of 3 to 6 days until syncytial cytopathic effect appears. Shell vial centrifugation cultures followed by DFA or immunoperoxidase staining using virus specific monoclonal antibodies significantly increases the sensitivity of the tissue culture technique and shortens the turnaround time for virus identification to 1 to 2 days [43-45].
The advantage of the tissue culture technique is that it is more sensitive than rapid antigen detection kits and that it provides the ability of further antigenic and genetic characterization of the amplified virus which can be used for the screening of epidemiological relevant mutations or for the confirmation of nosocomial transmission by sequence analysis [46-48].
Antigen Detection
Antigen detection assays include direct immunofluorescence assays (DFA), enzyme immunosorbent assays (EIA), chromatographic and optical immunoassays [49-54]. The DFA uses fluorescein-labelled antibodies that detect RSV antigen in epithelial cells in respiratory secretions and has the advantage that the immunofluorescence pattern of the infected cells can be directly examined by microscopy which provides additional confirmation of specificity. In the EIA, RSV antigen, if present, is captured by RSV-specific antibodies and will be detected by a second enzyme-linked antibody. Antigen detection kits are easy to perform and the results are available in a short time. For these reasons they are widely used in clinical practice. Currently available antigen detection kits in paediatric specimens have sensitivities of 72 to 94% and specificities of 95 to 100% as compared to cell culture (Table 1). However, in older children and adults, detection rates for EIA are extremely low with sensitivities of 0 to 20% (Tables 1 and 2), most likely because of the substantially lower viral titre and shorter virus shedding in a group of patients experiencing RSV reinfections [55]. The specificity of antigen detection kits may be significantly reduced, especially if used outside the epidemic periods, when the prevalence of the virus in the community is low and the rate of false positive results becomes relatively high [56-60]. Although numerous efforts are undertaken to improve the sensitivity and specificity of antigen detection kits, methods are less specific and far less sensitive than nucleic acid amplification assays [61-63].
Evaluation of RSV Rapid Antigen Detection Tests in Respiratory Specimens Obtained from Children and Adults with RSV Infection Confirmed by Cell Culture
| Assays | % Sensitivity | % Specificity | Positive Predictive Value | Negative Predictive Value | ||||
|---|---|---|---|---|---|---|---|---|
| Children n=108 | Adults n=41 | Children n=127 | Adults n=53 | Children n=84 | Adults n=34 | Children n=66 | Adults n=22 | |
| DFA | 93 | 100 | 97 | 97 | 95 | 80 | 96 | 100 |
| BD Directigen | 81 | 25 | 95 | 98 | 90 | 50 | 91 | 94 |
| BD Directigen EZ | 72 | 0 | 98 | 100 | 93 | 90 | 82 | |
| Binax Now | 94 | 0 | 100 | 100 | 100 | 96 | 94 | |
DFA, direct immunofluorescence assay (Merifluor RSV identification reagent, Meridian Bioscience Inc., Cincinnati, Ohio); BD Directigen, direct enzyme immunoassay and BD Directigen EZ (Becton Dickinson, Cockeysville, MD); Binax Now, rapid immunoassay (Binax, Inc., Portland, Maine), modified from [50].
Evaluation of RSV Rapid Antigen Detection Tests in Respiratory Specimens Obtained from Adults with RSV Infection Confirmed by Cell Culture and/or Serology and/or RT-PCR
| Assays | n Positive out of 60 Confirmed Infections | % Sensitivity | % Specificity | Positive Predictive Value | Negative Predictive Value |
|---|---|---|---|---|---|
| Cell culture | 28 | 46 | 100 | 100 | 95 |
| RT-PCR | 49 | 82 | 100 | 100 | 98 |
| DFA | 14 | 23 | 97 | 44 | 93 |
| VIDAS | 12 | 20 | 97 | 40 | 92 |
| BD Directigen | 6 | 10 | 97 | 25 | 92 |
DFA, direct immunofluorescence assay (Bartels (Bartels, Inc., Issaquah, WA); VIDAS, automated enzyme immunoassay (BioMerieux, Inc., Hazelwood, MI); Directigen, direct enzyme immunoassay (Becton Dickinson, Cockeysville, MD), modified from [58].
Nucleic Acid Tests (NATs)
Nucleic acid assays have revolutionized the diagnostic procedures in virology and are the most sensitive and specific methods for the detection of RSV, regardless of the patient population tested [58, 64-69]. Studies comparing molecular diagnostic assays to virus isolation in cell culture and to antigen detection assays have demonstrated superior sensitivity for nucleic acid tests [62, 63, 70-73] (Table 2) which leads to an approximately twofold increase of detection rates in infants with respiratory illness [71, 74]. Young children experiencing primary infection usually shed large quantities of RSV over a prolonged period of time. With the increasing number of subsequent infections, virus is shed in lower quantities for shorter times [75] due to the presence of secretory and humoral virus-specific antibodies influencing the degree of viral replication [76]. Therefore a decrease in the efficacy of RSV detection with increasing age of the patient has been reported in various studies [50, 56, 57, 70, 77-79]. Nevertheless molecular diagnostic assays are definitely also more sensitive for older age groups as a result of the lower virus production in these patients (Table 2, Fig. 3).
Of the different nucleic acid amplification techniques, reverse transcription polymerase chain reaction (RT-PCR) was the first and most frequently used nucleic acid-based assay [80-82]. In the last ten years, numerous in-house PCR protocols have been published for amplifying various gene segments of the RSV genome [70, 83-87] and, in addition, an increasing number of commercial RSV NAT kits are now available.
New PCR techniques, as for example the real-time PCR methods, have been developed. Real-time PCR assays that use fluorescent probes such as Taqman, molecular beacons and scorpion probes enable the simultaneous performance of amplification and detection and result in a considerable increase in the speed of RT-PCR with a turnaround time of a few hours. Protocols have also been designed for simultaneous amplification of RSV together with various other respiratory viruses which cause similar clinical symptoms. These multiplex PCR assays are able to identify a variety of different respiratory viruses simultaneously, either within a single tube or by parallel detection in a single PCR run. Using highly sensitive monoplex or multiplex PCR assays, it turned out that a significant proportion of up to 10-30% of respiratory illness cases and up to 50% of RSV-infections in infants represent mixed infections of 2 or more respiratory viruses [17, 24, 74, 88-90] (Fig. 2). The impact of a coinfection on the clinical course of illness still remains controversial. A significantly increased risk of more severe disease or of admission to a paediatric intensive care unit has been reported for dual as compared to single respiratory virus detection by some [91-93], but not by other studies [17, 74].
An important benefit of real-time PCR is that it allows quantification of viral nucleic acids present in a sample [66, 77]. The diagnostic value of the determination of viral loads in respiratory tract infections is still unclear, because respiratory specimens are difficult to standardize, especially with regard to the amount of virus or virus-infected cells within specimens and the non-standardized dilution of samples.
As far as RSV is concerned higher viral loads seem to correspond with a more severe clinical course of the disease [94, 95] and an increased likelihood of recurrence of wheezing [24]. In patients in whom multiple viruses are detected quantitative RT-PCR may help to discriminate between the virus actually causing the acute respiratory disease and those simultaneously detected but without a causative relationship to the actual clinical symptoms.
Determination of RSV-Specific Antibodies (Serology)
Testing for virus specific antibodies is not useful for the diagnosis of acute RSV-infection. A serologic response is usually not detectable in infants, despite severe RSV infection [75, 96]. Even when sophisticated tests for the detection of class specific antibodies are used, the infant’s own antibody response is barely detectable in the presence of maternally derived antibodies [97] and even in older children and groups of patients repeated infections are usually not associated with a detectable antibody response [75, 98]. Screening for RSV-specific antibodies is mostly performed to obtain seroepidemiologic information and for research purposes [99].
FUTURE TRENDS AND NEEDS FOR IMPROVEMENT
Future developments for the diagnosis of viral respiratory tract infection should enhance the development of cost effective, sensitive and rapid tests allowing the screening of at risk populations for all probable causative agents. RT-multiplex PCRs have been developed to use numerous primers within a single reaction tube to amplify nucleic acid fragments from different respiratory viral pathogens. Up to now data on the comparative analysis between multiplex reactions and mono-reactions on the same sample indicate a reduced sensitivity and specificity of the multiplex systems [80]. Therefore more research is needed to overcome the problems associated with the use of multiple sets of high concentration primers and to identify reaction conditions that can be combined in order to obtain maximal specificity with a minimal loss in sensitivity. Target-enriched multiplexing amplification and the use of padlock probe design may aid to overcome these technical problems [100]. In addition optimized extraction procedures, improved standardisation associated with more automation and different testing protocols for summer and winter months based on epidemiologic data will provide accurate and clinically meaningful results that will considerably improve diagnosis of respiratory infections and directly impact patient management.

