All published articles of this journal are available on ScienceDirect.

Characterization and Antimicrobial Resistance Profile of Prevalent Uropathogens: A Retrospective Analysis in Primary Care in Peru
Abstract
Background
Bacterial infections are a major cause of morbidity and mortality worldwide. In Peru, antimicrobial consumption and inappropriate prescribing are both common.
Objective
The objective of this study was to evaluate the characteristics and antimicrobial resistance profiles of prevalent uropathogens in primary care.
Materials and Methods
A retrospective cross-sectional analysis was performed using urine culture records processed between 2024 and 2025 from seven primary care facilities in the Callao region, Peru, serving a predominantly urban population with diverse socioeconomic backgrounds. Urine cultures were classified into three categories: susceptible, intermediate, or resistant. Antimicrobial susceptibility testing was interpreted according to disk diffusion breakpoints, following the guidelines of the Clinical and Laboratory Standards Institute (CLSI).
Results
The analysis included 1,685 cases, with a median age of 43 years (Min: 0, Max: 97, Q1: 25, Q3: 59, IQR: 34). Women accounted for 84.9% (n = 1,431) of the study population. Among the samples, 22.1% (n = 372) were positive, of which 89.5% (333/372) occurred in women (p = 0.007). The most frequently isolated species were Escherichia coli (63.4%), Enterococcus spp. (5.9%), and Klebsiella spp. (5.1%). The antimicrobials with the highest susceptibility rates were nitrofurantoin (93.8%) and amikacin (83.4%).
Discussion
Our findings confirm Escherichia coli as the main uropathogen in primary care and support the use of nitrofurantoin as first-line therapy. The observed resistance patterns highlight the need for careful antibiotic selection.
Conclusion
In primary care, one-fifth of urine samples tested positive for bacterial species. The most frequently isolated pathogens were Escherichia coli, Enterococcus spp., and Klebsiella spp. The agents with the highest susceptibility and lowest resistance rates were nitrofurantoin and amikacin, both of which are available in primary care settings. Periodic surveillance of antimicrobial susceptibility is essential to monitor bacterial resistance patterns.
1. INTRODUCTION
Bacterial infections represent a clinically significant cause of health loss worldwide. It is estimated that 13.7 million infection-related deaths occur annually, of which 7.7 million are associated with 33 bacterial pathogens, with more than half attributable to five pathogens: Staphylococcus aureus, Escherichia coli, Streptococcus pneumoniae, Klebsiella pneumoniae, and Pseudomonas aeruginosa [1]. Antimicrobial resistance (AMR) is one of the major threats to global public health and development [2, 3]. AMR is associated with 4.71 million deaths, 1.14 million of which are attributable to bacterial resistance [3]. In Latin America, the case fatality rate related to multidrug resistance reaches 45% [4].
Mortality attributable to AMR shows distinct age-related patterns; it decreases in children under five but is projected to rise among individuals over 70 years of age [3]. Globally, an estimated 4.95 million deaths were associated with antimicrobial resistance, of which 1.27 million were directly attributable to it, with the highest mortality observed in sub-Saharan Africa [5]. In China, infectious diseases and AMR pose a serious threat to public health, accounting for approximately 1.3 million and more than 600,000 deaths annually, respectively, representing 12.1% of all deaths [6].
The inappropriate and excessive use of antimicrobials in humans, animals, and plants is the main driver of the development of resistant pathogens [7]. However, reduced antibiotic prescribing in primary care has not been associated with an increased incidence of severe bacterial infections [8].
In Peru, both consumption and inappropriate prescribing of antimicrobials are high [9]. Self-medication is a common practice [10], primarily associated with the lack of prescription requirements in pharmacies [11]. In high-complexity hospital settings, the four most frequently used antimicrobials are ceftriaxone, vancomycin, meropenem, and imipenem [12]; in intensive care units, 74% of patients received antimicrobial prescriptions [13]. Additionally, amoxicillin (89%) and clindamycin (98%) are widely prescribed by endodontists [14].
Infections are among the leading causes of consultation in primary care [15], and urinary tract infections (UTIs) represent a significant social and healthcare burden [16]. Moreover, pregnant women in Latin America have a higher prevalence of UTIs [17]. The pathogens responsible for UTIs vary by region, making local data essential for infection control [16]. High levels of antibiotic resistance have been reported in Peruvian hospitals [12, 18, 19].
Understanding the resistance profile of prevalent uropathogens in primary care is highly relevant, as urinary tract infections are a common reason for medical consultation. Moreover, the effectiveness of empirical treatment relies on up-to-date local epidemiological data on susceptibility patterns. Generating evidence at the primary care level is essential to guide rational treatments, optimize patient clinical outcomes, and strengthen strategies for AMR surveillance and control. In this context, the present study seeks to answer the following question: What are the prevalent uropathogens and their antimicrobial resistance patterns in primary care in Peru? Therefore, the objective of this study is to evaluate the characteristics and resistance profile of prevalent uropathogens in this healthcare setting.
2. MATERIALS AND METHODS
2.1. Study Design and Data Source
A retrospective cross-sectional study was conducted using secondary data from urine culture records at the Reference Microbiology Laboratory of the North Health Network, Callao Region, Lima, Peru. The analysis included records from February 2024 to April 2025.
2.2. Study Population
The study population consisted of all urine culture records processed at the Reference Microbiology Laboratory for patients attending seven primary care facilities located in the districts of “Mi Perú” and “Ventanilla” (Callao Region, Peru).
2.3. Inclusion and Exclusion Criteria
A non-probabilistic convenience sampling approach was applied. Records were included if they met the following criteria: outpatients of both sexes and all ages with a positive urine culture (bacterial growth ≥ 105 CFU/mL) and a recorded antibiogram.
2.4. Identification and Antimicrobial Susceptibility
The antimicrobial susceptibility testing of the bacterial isolates was performed using the disk diffusion method, with interpretation based on the Clinical and Laboratory Standards Institute (CLSI) guidelines [20, 21], applicable at the time of testing. Isolated species were classified as susceptible, intermediate, or resistant for each evaluated antibiotic.
The following antibiotics were included: Amikacin (AMK), Amoxicillin/Clavulanate (AMC), Ampicillin (AMP), Aztreonam (ATM), Ceftazidime (CAZ), Cefazolin (CFZ), Cefadroxil (CFR), Cephalothin (CEF), Ciprofloxacin (CIP), Gentamicin (GEN), Gentamicin (GEN1=10), Gentamicin (GEN2=120), Gentamicin (GEN3), Ceftriaxone (CRO), Cefotaxime (CTX), Cefuroxime (CXM), Doxycycline (DOX), Ertapenem (ETP), Nitrofurantoin (NIT), Nitrofurantoin (NIT1=300), Nitrofurantoin (NIT2), Cefepime (FEP), Fosfomycin (FOS), Cefoxitin (FOX), Imipenem (IMI), Levofloxacin (LVX), Meropenem (MEM), Nalidixic Acid (NAL), Novobiocin (NOV), Norfloxacin (NOR), Oxacillin (OXA), Nifuroxazide (NFX), Ampicillin/Sulbactam (SAM), Trimethoprim/Sulfamethoxazole (SXT), and Piperacillin/ Tazobactam (TZP).
2.5. Data Analysis
Data processing and analysis were performed using RStudio (version 4.5.0) and edited in Microsoft Excel. Descriptive analysis included the creation of frequency tables and proportions to: (a) characterize the distribution of positive and negative urine cultures by sex and age group, (b) evaluate the frequency of isolated bacterial species, and (c) determine antimicrobial susceptibility profiles. For bivariate analysis, associations between categorical variables (sex vs. urine culture results and isolated species) were assessed using the Chi-square test. A significance level of p < 0.05 was set.
2.6. Ethical Considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki of the World Medical Association. The protocol was approved by the Ethics Committee of the University of Sciences and Humanities. Given the retrospective design using anonymized secondary data, informed consent was waived. Confidentiality was maintained by using numerical codes instead of personal identifiers.
3. RESULTS
A total of 1,697 urine culture records were reviewed, of which 12 were excluded due to incomplete or inconsistent data. The analysis included 1,685 cases, with a median age of 43 years (Min: 0, Max: 97, Q1: 25, Q3: 59, IQR: 34); 84.9% (n = 1,431) were female, and 15.1% (n = 254) were male. Among the samples, 22.1% (n = 372) were positive, with 89.5% (333/372) of positive cases occurring in women. A significantly higher proportion of positive cases was found among females (p = 0.007, Cramer’s V = 0.068), and positivity rates were also higher among older adults (p < 0.001, Cramer’s V = 0.138) (Table 1).
The proportion of positive results relative to the total sample was significantly higher in females (p = 0.007), with a frequency of 23.3% (n = 333) compared to 15.4% (n = 39) in males (Table 2). The five most frequently isolated species were Escherichia coli (63.4%), Enterococcus spp. (5.9%), Klebsiella spp. (5.1%), Staphylococcus aureus (4.3%), and Staphylococcus spp. (3%). Additionally, 3% of positive cases showed co-occurrence of Escherichia coli/Klebsiella spp. (Fig. 1).
| Variables | Total | Negative | Positive | p-value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Urine culture result | 1685 | 100 | 1313 | 77.9 | 372 | 22.1 | - |
| Sex | - | - | - | - | - | - | - |
| Female | 1431 | 100 | 1098 | 76.7 | 333 | 23.3 | 0.007 |
| Male | 254 | 100 | 215 | 84.6 | 39 | 15.4 | - |
| Age group (excluding NA) | - | - | - | - | - | - | - |
| Children/Adolescents | 174 | 100 | 154 | 88.5 | 20 | 11.5 | <0.001 |
| Young adults | 438 | 100 | 352 | 80.4 | 86 | 19.6 | - |
| Middle-aged adults | 414 | 100 | 329 | 79.5 | 85 | 20.5 | - |
| Older adults | 330 | 100 | 231 | 70 | 99 | 30 | - |
| Total | 1356 | 100 | 1066 | 78.6 | 290 | 21.4 | - |
| Variables | Total | - | Female | - | Male | - | p-value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | - | n | % | - | n | % | - | ||
| Total | 1685 | 100 | - | 1431 | 100 | - | 254 | 100 | - | - |
| Urine culture | - | - | - | - | - | - | - | - | - | - |
| Negative | 1313 | 77.9 | - | 1098 | 76.7 | - | 215 | 84.6 | - | 0.007 |
| Positive | 372 | 22.1 | - | 333 | 23.3 | - | 39 | 15.4 | - | - |
| Isolated species | - | - | - | - | - | - | - | - | - | - |
| Candida albicans | 3 | 0.8 | - | 3 | 0.9 | - | 0 | 0.0 | - | 0.052 |
| Candida glabrata | 1 | 0.3 | - | 1 | 0.3 | - | 0 | 0.0 | - | - |
| Candida krusei | 1 | 0.3 | - | 1 | 0.3 | - | 0 | 0.0 | - | - |
| Citrobacter spp. | 2 | 0.5 | - | 2 | 0.6 | - | 0 | 0.0 | - | - |
| Enterobacter spp. | 10 | 2.7 | - | 10 | 3.0 | - | 0 | 0.0 | - | - |
| Enterococcus spp. | 22 | 5.9 | - | 20 | 6.0 | - | 2 | 5.1 | - | - |
| Escherichia coli/Klebsiella spp. | 11 | 3.0 | - | 10 | 3.0 | - | 1 | 2.6 | - | - |
| Escherichia coli | 236 | 63.4 | - | 216 | 64.9 | - | 20 | 51.3 | - | - |
| Klebsiella oxytoca | 3 | 0.8 | - | 2 | 0.6 | - | 1 | 2.6 | - | - |
| Klebsiella pneumoniae | 9 | 2.4 | - | 7 | 2.1 | - | 2 | 5.1 | - | - |
| Klebsiella spp. | 19 | 5.1 | - | 13 | 3.9 | - | 6 | 15.4 | - | - |
| Proteus mirabilis | 4 | 1.1 | - | 4 | 1.2 | - | 0 | 0.0 | - | - |
| Proteus spp. | 10 | 2.7 | - | 9 | 2.7 | - | 1 | 2.6 | - | - |
| Pseudomonas spp. | 1 | 0.3 | - | 0 | 0.0 | - | 1 | 2.6 | - | - |
| Staphylococcus aureus | 16 | 4.3 | - | 13 | 3.9 | - | 3 | 7.7 | - | - |
| Staphylococcus epidermidis | 7 | 1.9 | - | 7 | 2.1 | - | 0 | 0.0 | - | - |
| Staphylococcus saprophyticus | 6 | 1.6 | - | 6 | 1.8 | - | 0 | 0.0 | - | - |
| Staphylococcus spp. | 11 | 3.0 | - | 9 | 2.7 | - | 2 | 5.1 | - | - |
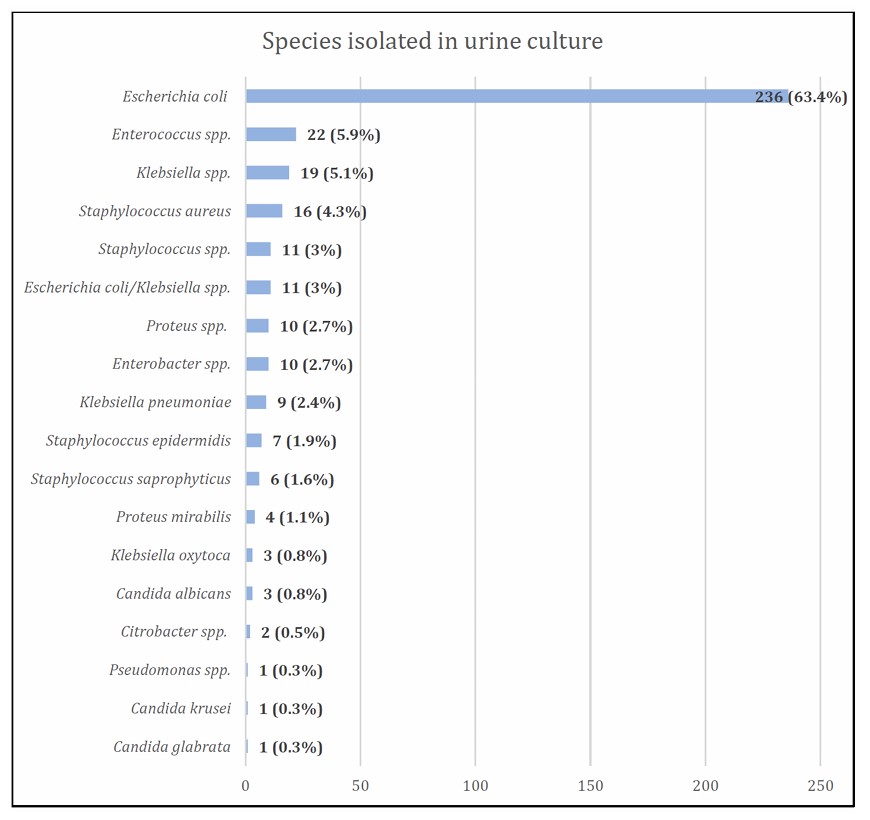
Frequency of species isolated in urine cultures.
No significant differences in isolated species were observed between sexes (p = 0.052). Among females, Escherichia coli and Enterococcus spp. were more frequent, while in males, Escherichia coli and Klebsiella spp. predominated (Table 2).
Regarding antimicrobial susceptibility, the agents with the highest frequency of susceptibility were nitrofurantoin (93.8%), meropenem (85.7%), amikacin (83.4%), imipenem (81.8%), and cefoxitin (80.9%) (Table 3) (Fig. 2).
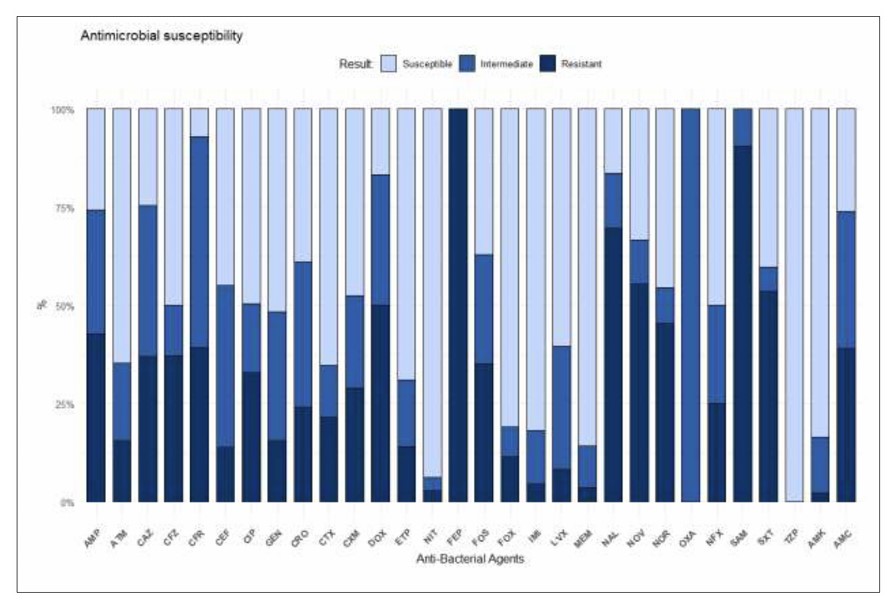
Antimicrobial susceptibility of isolated species.
| Anti-Bacterial Agents | Susceptible | - | Intermediate | - | Resistant | - | |||
|---|---|---|---|---|---|---|---|---|---|
| n | % | - | n | % | - | n | % | - | |
| Amikacin (AMK) | 247 | 83.4 | - | 42 | 14.2 | - | 7 | 2.4 | - |
| Amoxicillin/Clavulanate (AMC) | 42 | 26.1 | - | 56 | 34.8 | - | 63 | 39.1 | - |
| Ampicillin (AMP) | 9 | 25.7 | - | 11 | 31.4 | - | 15 | 42.9 | - |
| Aztreonam (ATM) | 75 | 64.7 | - | 23 | 19.8 | - | 18 | 15.5 | - |
| Ceftazidime (CAZ) | 37 | 24.5 | - | 58 | 38.4 | - | 56 | 37.1 | - |
| Cefazolin (CFZ) | 78 | 50.0 | - | 20 | 12.8 | - | 58 | 37.2 | - |
| Cefadroxil (CFR) | 2 | 7.1 | - | 15 | 53.6 | - | 11 | 39.3 | - |
| Cephalothin (CEF) | 13 | 44.8 | - | 12 | 41.4 | - | 4 | 13.8 | - |
| Ciprofloxacin (CIP) | 161 | 49.5 | - | 57 | 17.5 | - | 107 | 32.9 | - |
| Gentamicin (GEN) | 123 | 51.7 | - | 78 | 32.8 | - | 37 | 15.5 | - |
| Gentamicin (GEN1=10) | 1 | 50.0 | - | 0 | 0.0 | - | 1 | 50.0 | - |
| Gentamicin (GEN2=120) | 5 | 62.5 | - | 0 | 0.0 | - | 3 | 37.5 | - |
| Gentamicin (GEN3) | 117 | 51.1 | - | 78 | 34.1 | - | 34 | 14.8 | - |
| Ceftriaxone (CRO) | 55 | 39.0 | - | 52 | 36.9 | - | 34 | 24.1 | - |
| Cefotaxime (CTX) | 173 | 65.3 | - | 35 | 13.2 | - | 57 | 21.5 | - |
| Cefuroxime (CXM) | 128 | 47.6 | - | 63 | 23.4 | - | 78 | 29.0 | - |
| Doxycycline (DOX) | 1 | 16.7 | - | 2 | 33.3 | - | 3 | 50.0 | - |
| Ertapenem (ETP) | 69 | 69.0 | - | 17 | 17.0 | - | 14 | 14.0 | - |
| Nitrofurantoin (NIT1) | 32 | 28.6 | - | 59 | 52.7 | - | 21 | 18.8 | - |
| Nitrofurantoin (NIT2) | 196 | 93.8 | - | 7 | 3.3 | - | 6 | 2.9 | - |
| Cefepime (FEP) | 0 | 0.0 | - | 0 | 0.0 | - | 7 | 100.0 | - |
| Fosfomycin (FOS) | 95 | 37.1 | - | 71 | 27.7 | - | 90 | 35.2 | - |
| Cefoxitin (FOX) | 191 | 80.9 | - | 18 | 7.6 | - | 27 | 11.4 | - |
| Imipenem (IMI) | 18 | 81.8 | - | 3 | 13.6 | - | 1 | 4.5 | - |
| Levofloxacin (LVX) | 29 | 60.4 | - | 15 | 31.2 | - | 4 | 8.3 | - |
| Meropenem (MEM) | 24 | 85.7 | - | 3 | 10.7 | - | 1 | 3.6 | - |
| Nalidixic Acid (NAL) | 41 | 16.4 | - | 35 | 14.0 | - | 174 | 69.6 | - |
| Novobiocin (NOV) | 3 | 33.3 | - | 1 | 11.1 | - | 5 | 55.6 | - |
| Norfloxacin (NOR) | 10 | 45.5 | - | 2 | 9.1 | - | 10 | 45.5 | - |
| Oxacillin (OXA) | 0 | 0.0 | - | 1 | 100.0 | - | 0 | 0.0 | - |
| Nifuroxazide (NFX) | 4 | 50.0 | - | 2 | 25.0 | - | 2 | 25.0 | - |
| Ampicillin/Sulbactam (SAM) | 0 | 0.0 | - | 10 | 9.4 | - | 96 | 90.6 | - |
| Trimethoprim/Sulfamethoxazole (SXT) | 90 | 40.2 | - | 14 | 6.2 | - | 120 | 53.6 | - |
| Piperacillin/Tazobactam (TZP) | 1 | 100.0 | - | 0 | 0.0 | - | 0 | 0.0 | - |
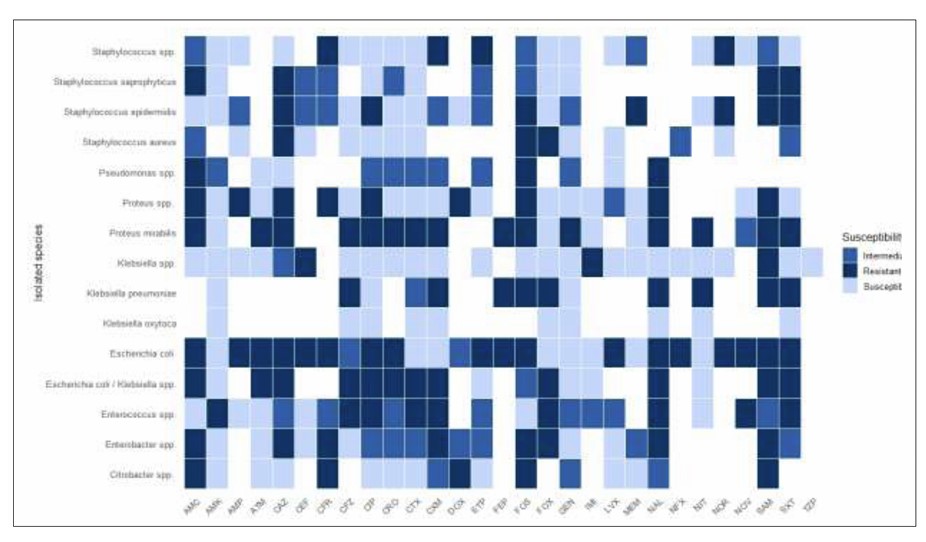
Isolated species and susceptibility to antibacterial agents.
Among the antimicrobial agents, amikacin was effective against most isolated species, except Enterococcus spp. and Pseudomonas spp. Nitrofurantoin was effective against most isolated species, except Klebsiella pneumoniae and Proteus mirabilis. Escherichia coli was susceptible to amikacin and nitrofurantoin, as well as to cefotaxime (CTX), cefuroxime (CXM), cefoxitin (FOX), gentamicin (GEN), imipenem (IMI), and meropenem (MEM). Enterococcus spp. was susceptible to amoxicillin/clavulanate (AMC), ampicillin (AMP), aztreonam (ATM), cephalexin (CEF), fosfomycin (FOS), and nitrofurantoin (NIT). Klebsiella spp. was susceptible to most tested antibiotics, except ceftazidime (CAZ), cephalexin (CEF), imipenem (IMI), and ampicillin/ sulbactam (SAM) (Fig. 3).
4. DISCUSSION
The present study aimed to evaluate the characteristics and resistance profile of prevalent uropathogens in primary care. In this regard, 22.1% of processed samples tested positive, with 89.5% of these cases occurring in women. The age group with the highest proportion of positive cases was older adults. Positive cases were significantly higher in women (p = 0.007).
The frequency of positive urine cultures in this study was lower than that reported in primary care settings in Spain (33.4%) [22], but higher than that recorded in Oman (10.7%) [23] and England (8.5%) [24]. In our study, positive cases occurred predominantly in women (p = 0.007), a finding consistent with other reports. In Oman, 92.8% of positive cultures were from females (p < 0.001), with additional associations observed for the presence of symptoms (p = 0.003) and pregnancy status (p = 0.001) [23].
UTIs predominantly affect women, with an approximate female-to-male ratio of 4:1 [25], and in premenopausal women, the risk can be 20 to 40 times higher [26]. Various risk factors promote infection and potential bacterial proliferation [27], including age, anatomical differences, and immunological and hormonal factors [26]. It is also important to note that, in our study, the majority of patients were female, which may partly account for this finding.
A positive culture does not necessarily indicate a UTI, as asymptomatic bacteriuria (ABU) is common in older adults and pregnant women [28]. Its clinical relevance lies in the increased risk of pyelonephritis and potential adverse pregnancy outcomes, such as preterm birth or low birth weight [29]. The incidence of asymptomatic bacteriuria increases with age and is more frequent in women, with a prevalence of 15%, although it can reach up to 50% in individuals residing in long-term care facilities [30]. In most cases, asymptomatic bacteriuria does not lead to UTIs, and screening and antibiotic treatment have not been shown to improve patient outcomes [30, 31, 32]. Individuals with ABU often receive unnecessary antibiotic treatment, posing a risk of adverse effects and antimicrobial resistance [33].
Screening and treatment of ABU are indicated only in pregnant women and in patients undergoing invasive urological procedures [25, 32, 34]. In pregnant women, evidence shows that treating ABU reduces the risk of symptomatic UTIs, low birth weight, and preterm birth [33]. Pregnant women in Latin America have a higher prevalence of bacteriuria, urinary tract infections, and pyelonephritis compared to pregnant women worldwide. This underscores the importance of universal urine culture screening during early prenatal care [17].
Within any microbiome, such as the urobiome, microbes can be classified as non-pathogenic, pathogenic, commensal, symbionts, colonizers, and pathobionts [28]. Increased water intake may prevent recurrent cystitis in premenopausal women by promoting dilution and flushing of bacteriuria, thereby reducing adhesion to uroepithelial cells, limiting nutrients for bacterial growth, and enhancing clearance [35].
In the present study, the most frequently isolated species were Escherichia coli (63.4%), Enterococcus spp. (5.9%), and Klebsiella spp. (5.1%). Additionally, 3% of positive cases showed co-occurrence of Escherichia coli/Klebsiella spp. In females, Escherichia coli and Enterococcus spp. were predominantly isolated, while in males, Escherichia coli and Klebsiella spp. Predominated.
Several studies agree that Escherichia coli is the main causative agent of UTIs [22, 36, 37, 38, 39, 40]. In Europe, studies in primary care in Spain reported this microorganism in 53.8% of cultures [22]; in England, E. coli was the most commonly isolated organism in UTI cases (73%) [39]; and in Sweden, among men with primary care UTIs, E. coli was detected in 62% of positive cultures [41]. In Asia, in Turkey, E. coli was the predominant pathogen, isolated in 61.2% of cases, followed by Klebsiella pneumoniae (13.3%) [40]. In West Africa, the most frequently isolated species were E. coli and Klebsiella spp., with frequencies of 49.4% and 13.9%, respectively [36]; in other regions, E. coli and Klebsiella spp. represented higher frequencies, reaching 71.2% and 27.3%, respectively [37]. In South America, in Bolivia, E. coli was the most prevalent pathogen in UTIs (86.6%) [38]; in Ecuador, UTIs were also mainly caused by E. coli and Klebsiella spp [42].
Reported frequencies of Klebsiella spp. in Latin America range from 5% to 12% [16]. In our study, Klebsiella spp. was detected in 5.1% of isolates, at the lower end of this regional range, possibly reflecting differences in populations, sample collection, or local epidemiology. In this study, the relatively high frequency of Enterococcus spp. (5.9%) is noteworthy; however, its presence alone does not indicate antimicrobial resistance, as susceptibility was assessed separately.
Recurrent UTIs are primarily caused by uropathogenic Escherichia coli, which resides in the intestines. This pathogen uses an adhesin called FimH to attach to colonic mucus and avoid elimination [43]. The FimH adhesin, covering type 1 pili, is a critical virulence factor in UTIs and facilitates intestinal colonization [44]. Bacterial composition differs by sex, with a lower proportion of UTIs caused by E. coli and a higher proportion caused by Pseudomonas aeruginosa in men compared to women [25].
Regarding antibiotic susceptibility, in our study, the agents with the highest frequency of susceptibility were nitrofurantoin (93.8%), meropenem (85.7%), amikacin (83.4%), imipenem (81.8%), and cefoxitin (80.9%). Among the antibacterial agents, amikacin was effective against most isolated species, except Enterococcus spp. and Pseudomonas spp. Nitrofurantoin was effective against most isolated species, except Klebsiella pneumoniae and Proteus mirabilis. Of the antibiotics mentioned, nitrofurantoin and amikacin are available at the primary care level in Peru [45].
Amikacin and nitrofurantoin showed the lowest resistance rates (<3%), whereas antibiotics, such as trimethoprim/sulfamethoxazole (53.6%), amoxicillin/ clavulanate (39.1%), ciprofloxacin (32.9%), and ceftriaxone (24.1%), which are widely used and available at the primary care level, exhibited high resistance frequencies. A study conducted in eight public hospitals across different regions of Peru reported high resistance percentages for ampicillin (77.1%), ciprofloxacin (74.3%), trimethoprim/ sulfamethoxazole (62.9%), cefepime (57.1%), cefuroxime (57.1%), and ampicillin/sulbactam (40%) [18]. These findings highlight that antimicrobial resistance in Peru is concerning, with high resistance rates observed in both primary care and hospital settings for the main antibiotics available within the public health system.
Internationally, Escherichia coli remains the primary causative agent of UTIs, with increasing resistance patterns. In Africa (Gabon), E. coli and Klebsiella pneumoniae exhibited resistance to beta-lactams, quinolones, and cotrimoxazole; resistance of E. coli to nitrofurantoin also showed a significant increase over the years [46]. In Sudan, E. coli was the primary uropathogenic bacterium identified, with 96% of isolates resistant to at least one antibiotic [47].
In South America, Bolivia, very high resistance rates (>50%) were reported for ampicillin, trimethoprim-sulfamethoxazole, and fluoroquinolones, high resistance rates (>20%) for amoxicillin-clavulanate, third-generation cephalosporins, and gentamicin, while lower resistance rates (<10%) were observed for nitrofurantoin and fosfomycin [38]. In Ecuador, among women with UTIs, cotrimoxazole was the least effective antibiotic, with 61% of isolates resistant [42]. In Europe, England, resistance to trimethoprim was high (27%), with lower resistance to cephalexin (8.3%) and nitrofurantoin (8.8%) [39]; in Sweden, resistance to ciprofloxacin was 9%, and resistance to trimethoprim was 17% [41]. In Asia (Turkey), high resistance rates were observed for ampicillin (67.4% in E. coli and 100% in Klebsiella), TMP-SMX (33.2% in E. coli and 30% in Klebsiella), and cefixime (45.3% in E. coli) [40]. Global mapping of community-acquired uropathogenic E. coli susceptibility shows that antimicrobial susceptibility varies between countries. In most centers, susceptibility to oral antimicrobials was low: cotrimoxazole <60%, amoxicillin-clavulanate <70%, first-generation cephalosporins <50%, and fluoroquinolones <60% [48].
These findings reflect a global trend of increasing resistance to certain antibiotics, with regional variations highlighting the need for continuous surveillance and rational antimicrobial use. The most significant upward trends over the past 30 years were reported for sulfamethoxazole/trimethoprim (SXT) (R2 = 73.24%, p < 0.001), ciprofloxacin (R2 = 61.44%, p < 0.001), and third-generation cephalosporins (R2 = 18.49%, p < 0.001) [37]. In the African context, the overall prevalence of multidrug-resistant (MDR) bacteria, defined as bacteria resistant to three antibiotics from three different families, reaches 59% (95% CI: 48–69%), with higher prevalence in nosocomial infections (65%, 95% CI: 45–81%) than in community-acquired infections (53%, 95% CI: 31–74%). MDR prevalence is reported mainly in urine samples (72%, 95% CI: 57–84%) [36].
Of UTI episodes, 78% involve an antibiotic prescription, with nitrofurantoin being the most commonly prescribed agent [24]. Nitrofurantoin, used for more than seven decades, has relatively low resistance levels [49]. In Sweden, Escherichia coli resistance to nitrofurantoin was 1% [41]. However, in a study conducted across 37 centers in Turkey, the region with the highest nitrofurantoin resistance was identified as Eastern Anatolia, with a rate of 35.7% [50].
Nitrofurantoin remains effective for the treatment of uncomplicated lower UTIs. The presence of multiple mechanisms of action for nitrofurantoin may explain the limited ability of bacteria to develop resistance to it [49]. Although generally effective and safe, nitrofurantoin can cause rare but severe toxicity, including reversible acute pneumonitis, chronic pulmonary fibrosis, fulminant hepatitis, and systemic inflammatory reactions [51, 52].
Global mapping of antimicrobial susceptibility of uropathogenic Escherichia coli highlights nitrofurantoin (89%) and fosfomycin (96%) as empirical treatment options worldwide. Injectable antibiotics showed better performance: piperacillin-tazobactam >70% and amikacin and meropenem >80% [48]. In Turkey, amikacin exhibited the lowest resistance among all pathogens, with only 0.9% resistance in E. coli [40]. These findings are consistent with our study, in which amikacin and nitrofurantoin showed the lowest resistance rates (<3%) and are widely available antibiotics in Peru [45], supporting their use as first-line options for uncomplicated UTIs and certain manageable cases of complicated UTIs at primary care facilities with adequate capacity.
The results of this study should be interpreted considering the following limitations: The analysis was based on secondary data, without access to relevant clinical information, such as comorbidities, gestational status, the reason for the urine culture request, or whether it was part of post-treatment follow-up. Another limitation was the heterogeneity in the source of antibiotic diffusion disks, as they were not obtained from a single supplier during the study period, which may have influenced susceptibility percentages. In particular, some nitrofurantoin disks came from an unidentified supplier, as noted by the laboratory.
Data on extended-spectrum beta-lactamase (ESBL) testing were also unavailable, which would have enhanced the study by enabling a more detailed analysis of antimicrobial resistance. This lack of information was likely due to limited resources and laboratory capacity.
Despite these limitations, the study included a considerable and representative sample from the Callao region, providing useful evidence for therapeutic decision-making at the primary care level.
CONCLUSION
At the primary care level, 1 in 5 urine samples tested positive for bacterial species, primarily among females and older adults. The most frequently isolated species in both women and men were Escherichia coli, Enterococcus spp., and Klebsiella spp. Additionally, co-occurrence of Escherichia coli/Klebsiella spp. was observed in 3% of positive cultures. In females, E. coli and Enterococcus spp. were the predominant isolates, whereas in males, E. coli and Klebsiella spp. Predominated.
Regarding antibiotic susceptibility, the agents with the highest frequency of susceptibility and lowest resistance rates were nitrofurantoin and amikacin. These antibiotics are available at the primary care level and can be used in the management of urinary tract infections. The results of this study provide valuable guidance for empirical antibiotic prescribing by primary care physicians, enabling more informed treatment decisions and optimizing patient outcomes. Additionally, the implementation of antimicrobial stewardship programs at the primary care level is recommended to optimize antibiotic use, reduce the emergence of resistance, and complement ongoing surveillance efforts.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: J.M. and E.H.C.: Study conception and design; E.H.C.: Data collection; J.M.: Analysis and interpretation of results; J.M.: Draft manuscript; E.H.C.: Critical review and technical precision. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AMR | = Antimicrobial resistance |
| CFU | = Colony-Forming Units |
| CLSI | = Clinical and Laboratory Standards Institute |
| IQR | = Interquartile range |
| MDR | = Multidrug resistant |
| Q1 | = 25th percentile |
| Q3 | = 75th percentile |
| UTIs | = Urinary tract infections |
| 95%CI | = 95% confidence interval |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The protocol was approved by the Ethics Committee of the University of Sciences and Humanities (CEI Act No. 114, Code: 076-2025).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2024.
CONSENT FOR PUBLICATION
Given the retrospective design using anonymized secondary data, informed consent was waived.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from https://doi.org/10.5281/zenodo.17195344.
FUNDING
The study was co-funded by the Research Directorate of the University of Sciences and Humanities (UCH), Lima, Peru.
ACKNOWLEDGEMENTS
The authors would like to sincerely thank Rosa del Pilar Zanabria Ruiz for her valuable assistance in preparing the data.

