All published articles of this journal are available on ScienceDirect.

A Review of Comparative Strategies Against Pneumonia: Vaccine and Antibiotic Resistance Mitigation
Authors Info & Affiliations
Abstract
Introduction/Background
Pneumonia remains a significant global health problem, worsened by the emergence of multidrug-resistant bacterial strains.
Aims and Objectives
This review aims to analyze the role of DNA vaccines in combating pneumonia, comparing them with mRNA vaccines and other innovations in vaccine technology to mitigate this issue.
Methods
The research on DNA and mRNA vaccines for pneumonia and their potential to lower antibiotic resistance was studied in this review. A thorough search was carried out in PubMed and Google Scholar using keywords like “pneumonia,” “vaccines,” “DNA vaccines,” “mRNA vaccines,” and “antibiotic resistance.” Additionally, we have also used Web of Science, Scopus, and DOAJ. Title/abstract and full text studies were evaluated in two phases. Preclinical and clinical research, reviews, and meta-analyses assessing the safety, immunogenicity, effectiveness, or influence on antibiotic resistance were among the articles that were used. Letters, conference abstracts, editorials, and irrelevant research were not included. An overview of current advances, obstacles, and public health potential was provided by examining data on vaccination type, pathogen target, delivery mechanism, research design, and major findings.
Results
Findings indicate that DNA vaccines encoding pneumococcal proteins effectively induce both humoral and cellular immunity, thereby reducing the dependence on antibiotics and slowing the development of resistance. Challenges, such as low immunogenicity and weak antibody responses, were identified, requiring improvements in adjuvant formulations and delivery mechanisms. An analysis of delivery systems, particularly highlighting lipid nanoparticles, which have demonstrated significant success in mRNA vaccines, revealed their potential for enhancing DNA vaccine applications due to high efficiency and biocompatibility. LNP-based systems offer superior antigen stability and immune response for DNA vaccines, while intramuscular injection remains the most accessible method for large-scale immunization. Quantitative data highlights efficacy rates for pneumococcal vaccines and alarming trends in S. pneumoniae antibiotic resistance.
Discussion
DNA vaccines are a promising approach to control pneumonia and reduce antibiotic resistance by stimulating both humoral and cellular immune responses against pathogens, such as Streptococcus pneumoniae. Studies show that DNA vaccines encoding pneumococcal proteins can lower infection severity and antibiotic use; however, limited immunogenicity in humans remains a key challenge. Enhancements through delivery mechanisms, especially lipid nanoparticles (LNPs), have been shown to strengthen antigen expression and immune activation. Compared with mRNA vaccines, DNA vaccines are more stable, cost-effective, and easier to store, while mRNA vaccines offer higher immunogenicity but require cold-chain storage. Continued advancements in delivery systems, adjuvant technologies, and clinical evaluation are essential to maximize their public health impact.
Conclusion
Despite their current limitations, DNA vaccines demonstrate significant potential in mitigating antibiotic resistance and reducing pneumonia-related mortality. Additionally, when compared with mRNA vaccines, they also appear well-suited for combating pneumonia pathogens. Continued research and development in delivery systems and adjuvant technologies are crucial to overcome existing challenges and fully realize the therapeutic promise of DNA and mRNA vaccines in public health.
1. INTRODUCTION
Vaccination is one of the most impressive applications of immunological principles to human health. Regular evaluations of vaccine efficacy are required, with safety maintaining the top priority. DNA vaccines are a simple yet effective way to induce broad immune responses. These vaccines create the antigen of interest internally by allowing microbial antigens to be expressed within host cells that contain the plasmid. This mechanism has the specific advantage of increasing the presentation of antigen via the main histocompatibility complex, hence promoting immune activation [1]. DNA vaccines, developed in the 1990s, stimulate cellular and humoral immune responses. They consist of a DNA plasmid that encodes a pathogenic peptide under a eukaryotic promoter and have demonstrated efficacy in animal trials. Four are licensed for veterinary usage. Though research into bacterial illnesses is limited, the early results are encouraging. Their safety, adaptability, and efficiency make them useful for addressing various diseases [2].
This study emphasizes the fundamental benefits of plasmid DNA-based vaccines, including their ability to manufacture antigens within the host and their straightforward, pathogen-free growth process. Recombinant DNA technology is used to create DNA vaccines, which mainly use bacterial plasmids to transfer genes encoding antigens into host cells. Without using live or attenuated viruses, this method elicits robust humoral and cellular immune responses, which makes the procedure intrinsically safer and more reliable [3]. Plasmid DNA vaccines are easier to make, thermostable, and scalable, which is a significant benefit over first- and second-generation vaccines [4]. The approval of four DNA-based treatments across species proves their efficacy while advances in delivery systems and excellent outcomes in human studies highlight the possibilities for DNA as an adaptable weapon for human and animal health [5]. Advantages over standard vaccines include the following:
- Production does not require live or virulent pathogens.
- Efficient and adaptable generation of emerging and pandemic diseases.
There is potential for tailored vaccines, especially tumor-specific therapy [2].
Crucially, DNA vaccines have demonstrated the ability to activate cytotoxic CD8+ T lymphocytes as well as CD4+ helper T cells, providing all-encompassing immune protection. Strong safety profiles and good immunogenicity in humans and animals have been shown by these vaccines in preclinical and clinical investigations [6]. Furthermore, new developments like liposomal encapsulation, electroporation, and nanoparticle-based administration have significantly increased their efficacy at lower dosages. These characteristics are especially important for respiratory infections that require both mucosal and systemic defense, such as pneumonia [7].
Additionally, DNA vaccination platforms offer a tactical edge in combating the problem of multidrug-resistant bacteria. DNA vaccines provide a more flexible option as conventional inactivated and live-attenuated vaccinations become less effective against germs that are resistant to antibiotics, like MDR Mycobacterium TB [8].
Mycobacterium tuberculosis is one of the most dangerous human pathogens. Tuberculosis (TB) causes almost 2 million deaths each year, with 8–10 million new active cases reported annually. Developing vaccines to prevent TB infection is, now, a global health necessity. The current vaccines available provide only half protection, mainly against TB meningitis and other forms of childhood TB, but their efficiency against pulmonary TB is lower, and they fail to provide lifelong immunity. This restraint has driven ongoing efforts to create new TB vaccines. A major problem in this process has been the limited diversity of antigens included in vaccines and the variability in immune responses among individuals with TB. Current strategies now focus on expanding the spectrum of antigens and enhancing the range of immune responses triggered by vaccination. Over the past two decades, progress has been made, with some TB vaccine candidates advancing to phase III clinical trials [9].
Highly conserved epitopes can be identified and encoded into DNA plasmids using reverse vaccinology and immune-informatics, resulting in multi-epitope vaccinations that offer more comprehensive protection and reduce the need for antibiotic intervention after infection [8].
This proactive strategy not only slows the spread of antibiotic resistance but also dramatically lowers treatment failure-related mortality and healthcare expenses. The ability of DNA vaccines to safeguard susceptible groups is yet another strong advantage. In preliminary research, nucleic acid-based vaccines have demonstrated positive immune responses in older adults, who are especially vulnerable to pneumonia and frequently react badly to traditional vaccinations. Due to their modularity, antigen sequences and delivery systems can be tailored to enhance immune responses in high-risk populations [10].
To sum up, DNA plasmid vaccinations present a very promising approach to combating AMR and pneumonia. Their broad immunological coverage, ease of manufacture, safety, and quick development give them significant advantages over conventional vaccination platforms. These next-generation vaccines are anticipated to play a key role in international public health initiatives for the prevention and control of pneumonia as biotechnology develops, especially in light of the growing medication resistance. Effective prophylaxis is critically needed, as seen by the surge in respiratory illnesses that are easily spread and microorganisms that are resistant to antibiotics [11]. A promising non-invasive treatment that can produce robust and long-lasting immune responses in model animals is intranasal DNA vaccinations. Although they work well in veterinary settings, their immunogenicity needs to be enhanced for human usage. To increase the effectiveness, tactics like focusing on antigen-presenting cells and developing efficient delivery mechanisms are essential. Compared to conventional vaccines, DNA vaccines have stability, lower production costs, and a lower chance of viral mutations and antigen mis-folding. A broad framework for creating vaccines against infectious diseases could be established by optimizing intranasal administration [12]. Streptococcus pneumoniae is responsible for pneumonia caused by bacteria, medial otitis, and meningitis, and it has 90 known serotypes [13].
Current PS-based vaccines include 23 serotypes; however, they have limited worldwide effectiveness and poor responsiveness in kids and the elderly. While conjugate vaccines boost responses, their high cost makes them unsuitable for use in developing nations. PsaA, a stable manganese permease protein, and PspA, a lactoferrin-binding protein having an antigenic variant, are attractive vaccine targets. Studies demonstrate that mixing PsaA and PspA improves resistance to infectious diseases. DNA vaccines, which provide combined humoral and cellular protection at an economical cost, were tested against PsaA and shortened PspA. They showed excellent antigen expression and powerful immune responses, indicating that they could provide widespread pneumococcal protection [14].
Table 1 shows different DNA vaccines made for pneumonia-causing germs. It lists the target antigens, delivery methods, and the stage of the research. It also gives short notes and references for each vaccine approach.
| Target Pathogen | Antigen |
Delivery Method / Platform |
Development Stage | Key Findings | Reference(s) |
|---|---|---|---|---|---|
| Streptococcus pneumoniae | Pneumococcal Surface Protein A (PspA) | Influenza virus vector (expressing PspA DNA) | Preclinical | Intranasal administration provided protection against nasal colonization. |
[15] |
| Streptococcus pneumoniae | PsaA and PspA mix | Method not specified | Preclinical | Historical studies show protection. | [15] |
| Various (including S. pneumoniae) | General DNA Vaccine Platforms | Electroporation, Lipid Nanoparticles (LNPs) | Platform Technology | Research focuses on improving immunogenicity and delivery systems. | [16] |
| SARS-CoV-2 (With potential Klebsiella pneumoniae application) |
IMNN-101 (DNA vaccine against SARS-CoV-2- 2) |
Electroporation | Phase 1 Clinical | Developed primarily for COVID-19; The pipeline suggests future use against K. pneumoniae. |
[17, 18] |
Since the pathogen was discovered in 1881, the development of pneumococcal vaccines has changed. Initially, vaccines employed heat-killed pneumococci [19], but later switched to serotype-specific capsule polysaccharides (CPS). After the discovery of penicillin, progress stalled until Robert Austrian's work produced PPSV23 in 1983, which covered 23 serotypes and opened the door to pneumococcal conjugate vaccinations (PCVs). These are now essential in childhood immunization initiatives and reduce illness in children as well as in high-risk adults. Having undergone this advancement, however, the development of a vaccine that is independent of serotypes remains a crucial and difficult goal [20, 21]. To protect against pneumonia-causing bacteria, the study employs a septicemia model to evaluate the effectiveness of DNA vaccines expressing genetically detoxified pneumolysin. The findings highlight the need to tailor vaccination procedures to specific antigens and anticipated immune responses, but they also suggest that DNA vaccines are ineffective for pneumolysin-based immunization due to insufficient neutralizing antibody production [22, 23]. Weak antibody responses, low immunogenicity, and limited efficacy in producing protective immunity are some obstacles to discovering DNA-based vaccines against Streptococcus pneumoniae [24]. DNA-based vaccinations encoding pneumocystis, including pneumolysin, have produced insufficient neutralizing antibodies, limiting their effectiveness, especially in intraperitoneal challenge animals. The prime-boost method, which combines DNA and recombinant protein vaccinations, has also been shown to be ineffective [25].
Antigens, such as pneumolysin do not regularly elicit significant protective responses, but PspA does. Furthermore, because different antigens elicit varied immune responses, vaccination techniques must be tailored to target specific antigens. These limitations underscore the need for more studies to enhance S. pneumoniae DNA vaccine development [26, 27].
2. METHODOLOGY
This review was performed using a systematic approach to collect, analyze, and summarize existing literature related to DNA and mRNA vaccines against pneumonia, with particular focus on their contribution to reducing antibiotic resistance.
An extensive literature search was performed across several scientific databases, including PubMed, Scopus, Web of Science, Google Scholar, and DOAJ. The search terms used were combinations of the following keywords: “pneumonia,” “respiratory infections,” “DNA vaccines,” “mRNA vaccines,” “antibiotic resistance,” and “multidrug-resistant bacteria.” Publications from 2010 to 2025 were thoroughly studied and reviewed. The search highlighted preclinical and clinical studies, as well as reviews and meta-analyses that discussed the safety, immunogenicity, and effectiveness of DNA and mRNA vaccines in relation to pneumonia.
Studies were included if they focused on DNA or mRNA vaccines targeting pneumonia-causing pathogens, reported immune responses, delivery systems, or adjuvant applications related to vaccine development, and further addressed the impact of vaccination on antibiotic consumption or antimicrobial resistance. All recovered studies were thoroughly screened first by their titles and abstracts to remove unrelated studies. Duplicate entries were excluded. To maintain fairness, two reviewers evaluated the studies, and any differences were resolved through discussion until an agreement was reached.
From the eligible studies, data were extracted regarding the type of vaccine (DNA or mRNA), target pathogen and antigen, delivery systems used, and key outcomes related to immune response or antibiotic resistance.
The collected information was summarized and presented in tables to explain current vaccine strategies and innovations (as shown in Tables 1 and 2).
| Adjuvant Type / Strategy | Mechanism of Action |
Advantages of DNA Vaccines |
Disadvantages / Challenges | Recent Reference(s) |
|---|---|---|---|---|
|
Plasmid-Encoded Adjuvants |
- | - | - | - |
| - Cytokines (e.g., GM- CSF, IL-12, IL-23) |
Co-expressed with antigen; modulate immune cell recruitment, activation, and differentiation. (e.g., Th1 bias). |
Co- localization of antigen and adjuvant; immune response tailoring. | Risk of systemic toxicity; dosage control is complex; plasmid engineering required. | [52, 53] |
| - Chemokines | Co-expressed to recruit APCs and enhance immune infiltration at Vaccination Site. |
Boosts local immune cell density and antigen uptake. |
Off-target effects; tight regulation of expression needed. | [10] |
|
Co-administered Adjuvants |
- | - | - | - |
| - TLR Agonists (e.g., CpG ODNs) | Activate PRRs like TLR9 on innate immune cells → cytokine secretion and adaptive priming. |
Potent innate activation; Th1-biased response; enhances cellular immunity. | Requires co-delivery system; can cause systemic inflammation. | [10, 54] |
|
Delivery Systems as Adjuvants |
- | - | - | - |
| - Lipid Nanoparticles (LNPs) | Protect DNA; facilitate cellular uptake; activate innate pathways (e.g., STING, TLRs). | Dual function (delivery + adjuvancy); enhances DNA stability & transfection. |
Formulation complexity; risk of inflammation; optimization ongoing. | [10, 55] |
| - Polymeric Nanoparticles (e.g., PEI, PLGA, PBAE) | Condense and protect DNA; enhance uptake; some polymers stimulate immunity. |
Tunable features; potential for controlled release. | Toxicity risks based on polymer type/concentration; formulation must be optimized. | [10, 56] |
| - Electroporation (EP) | Physically induces pores in membranes to facilitate DNA entry; causes local inflammation. | Highly improves in vivo NA uptake and immune response. | Needs electroporation device; may cause pain or variable efficiency. | [10, 16] |
| Molecular Adjuvants | - | - | - | - |
| - Co-stimulatory Molecules (e.g., CD40L) | Enhances activation of T and B cells; improves DC maturation when encoded or co-delivered. |
Directly boosts adaptive immunity (T/B cells). | Must be accurately expressed and targeted to avoid off-target effects. | [57] |
| Traditional Adjuvants | - | - | - | - |
| - Alum, Emulsions (e.g., MF59) | Create depot effect (Alum) or enhance uptake (MF59); primarily used in protein- based vaccines. |
Established safety; MF59 stimulates robust responses. | Not ideal with naked DNA; potential incompatibility with delivery methods; Alum biases Th2. | [10, 58, 59] |
A qualitative synthesis method was used to compare and understand the findings. Studies were classified according to vaccine type, mode of delivery, and research focus, including efficacy, safety, or contributions to antimicrobial resistance reduction. The main focus was on finding improvements in DNA vaccine performance and comparing their outcomes with those of mRNA vaccines.
As this study is based solely on published research, no human or animal experimentation was involved, and ethical approval was not required. All the data used were obtained from reliable, peer-reviewed, and publicly accessible sources.
3. QUANTITATIVE EVIDENCE ON VACCINE EFFICACY AND ANTIBIOTIC RESISTANCE
The growth and distribution of pneumococcal vaccines are serious strategies to fight pneumonia. The efficacy of these vaccines and the prevalence of resistance are supported by the following data.
3.1. Vaccine Efficacy
Multiple studies have measured the effectiveness of pneumococcal vaccines. For instance, the 13-valent pneumococcal conjugate vaccine (PCV13) has shown some impact. A study found that PCV13 had an adjusted vaccine effectiveness of 10.0% against pneumonia in adults [28]. A meta-analysis reported that PCV13 vaccination reduced the occurrence of vaccine-type invasive pneumococcal disease (IPD) in adults aged more than or equal to 65 years by 61.5% [29].
The 23-valent pneumococcal polysaccharide vaccine (PPSV23) has also been examined, with more diverse results. A meta-analysis stated a pooled vaccine efficacy of 63% against IPD due to any serotype [30], while another study showed less effectiveness of 2% against PPSV23-type pneumococcal pneumonia in adults aged ≥65 years [31].
3.2. Antibiotic Resistance in Streptococcus Pneumoniae
Antibiotic resistance in Streptococcus pneumoniae is a major global health threat. Surveillance data show a high occurrence of resistance to commonly prescribed antibiotics. In the United States, it is estimated that more than 2 in 5 S. pneumoniae infections are caused by a strain resistant to at least one antibiotic [32].
A study investigating trends in the United States found that roughly 39.9% of S. pneumoniae isolates were resistant to macrolides, such as erythromycin, and 39.6% were resistant to penicillin [33]. In certain regions, the incidence of penicillin resistance has been reported to be as high as 45% [34]. These high rates of resistance limit treatment choices and highlight the importance of vaccination as a key prevention approach.
4. INNOVATIONS IN DNA VACCINE TECHNOLOGY
4.1. Combining DNA Vaccines with Advanced Delivery Mechanisms
DNA vaccines involve introducing genetic material encoding antigens into the host, leading to antigen expression and eliciting an immune response [35]. They are known for their stability, ease of production, and rapid adaptability to emerging pathogens [36-38]. Nanoparticle carriers, such as lipid nanoparticles (LNPs) and polymer-based nanoparticles, play a crucial role in enhancing the delivery of DNA vaccines. These carriers protect DNA from enzymatic degradation in the extracellular environment, ensuring it reaches target cells intact. Once delivered, nanoparticles improve the uptake of DNA by antigen-presenting cells (APCs), leading to a robust immune response. Lipid nanoparticles, already proven successful in mRNA vaccines like the COVID-19 vaccines, are being actively explored for DNA vaccine applications due to their high efficiency and biocompatibility [39]. Electroporation is a delivery technique that uses brief electrical pulses to permeabilize cell membranes temporarily, facilitating the direct uptake of DNA into cells. This method significantly enhances the efficiency of DNA entry, resulting in increased antigen expression and a stronger immune response. Electroporation is particularly valuable for DNA vaccines as it bypasses many cellular barriers, ensuring effective transfection and immunogenicity [40]. Injectable hydrogel systems represent an innovative delivery platform for DNA vaccines. These hydrogels can encapsulate DNA, offering controlled and sustained release at the site of administration. This prolonged antigen exposure promotes a stronger and more durable immune response. Hydrogels are biocompatible and can be engineered to release DNA in response to specific environmental triggers, making them a versatile option for vaccine delivery [41].
4.2. Use of Adjuvants to Enhance Immunogenicity
Adjuvants are critical components in modern vaccines, designed to amplify and extend the immune response to an antigen. They work by activating innate immunity, enhancing antigen presentation, and stimulating the adaptive immune system, which collectively improve the magnitude and durability of the immune response. By modulating immune pathways, adjuvants allow vaccines to achieve stronger protection with smaller antigen doses, improving efficiency and cost-effectiveness [42]. Their role is particularly vital in DNA vaccines, where adjuvants can compensate for the comparatively low immunogenicity of DNA as a vaccine platform [43].
4.3. Types of Adjuvants in DNA Vaccines
Alum-based adjuvants are among the oldest and most widely used in vaccines, inducing a depot effect that slowly releases antigens and promotes the activation of antigen-presenting cells (APCs). This sustained antigen exposure enhances the overall immune response. While traditionally used in protein-based vaccines, alum-based adjuvants are now under investigation for use in DNA vaccines to improve their immunogenicity and facilitate robust antibody production [44].
TLR agonists mimic pathogen-associated molecular patterns (PAMPs) to stimulate innate immunity via toll-like receptors. CpG oligodeoxynucleotides (CpG ODNs), for example, target TLR9 to enhance the immunogenicity of DNA vaccines by activating dendritic cells and promoting T-helper cell responses. This approach has shown promise in preclinical studies, demonstrating significant enhancement of both humoral and cellular immunity [45].
MF59, a squalene-based oil-in-water emulsion, is a well-known adjuvant that facilitates antigen uptake by APCs, leading to a robust immune response. Its efficacy has been demonstrated in various vaccine platforms and is being explored for DNA vaccine applications. MF59 is particularly effective at inducing a balanced Th1 and Th2 immune response, critical for comprehensive immunity [46, 47].
Nanoparticles as adjuvant carriers offer dual functionality by protecting DNA and delivering adjuvant molecules to APCs simultaneously. This co-delivery mechanism ensures optimal activation of the immune system while enhancing the stability and bioavailability of DNA vaccines. Lipid nanoparticles, which played a key role in mRNA vaccine success, are now being adapted to DNA vaccines to improve their performance [48-50].
Cytokine adjuvants, such as interleukin-23 (IL-23) and granulocyte-macrophage colony-stimulating factor (GM-CSF), are co-delivered with DNA vaccines to modulate immune responses. These cytokines enhance the activation and proliferation of T cells, promoting a strong and sustained cellular immune response. This approach is particularly valuable in vaccines targeting intracellular pathogens and cancers, where T-cell-mediated immunity is crucial [51].
In the following Table 2, we can see different adjuvants and delivery methods used to increase the efficacy of DNA vaccines.
5. INTERPLAY BETWEEN VACCINE IMMUNITY AND ANTIBIOTIC RESISTANCE
5.1. Synergistic Impact
Vaccines play a pivotal role in reducing the incidence of infections that would otherwise require antibiotic treatment. By preventing bacterial infections, vaccines decrease the overall demand for antibiotics, which in turn reduces the risk of misuse and overuse —key drivers of antibiotic resistance [60]. For example, the widespread use of vaccines targeting viral respiratory infections, such as influenza vaccines, indirectly reduces secondary bacterial infections like pneumonia, diminishing the need for antibiotics [61].
In contrast, vaccines against bacterial pathogens, such as Haemophilus influenzae type b (Hib) and Streptococcus pneumoniae, directly prevent diseases that would necessitate antibiotic therapy [62]. By curbing infections at their source, vaccines reduce the opportunity for bacteria to be exposed to antibiotics and develop resistance. This is particularly significant in regions with high rates of antibiotic misuse, where vaccination programs can serve as a critical intervention to slow the spread of resistant strains [60]. The introduction of vaccines targeting multidrug-resis tant organisms, such as typhoid conjugate vaccines, exem plifies how immunization can act as a strategic measure against the global threat of antibiotic resistance [63].
5.2. Selective Pressures and Adaptation
While vaccines are powerful tools for disease prevention, their use can exert selective pressures on pathogens, potentially leading to evolutionary adaptations. For example, pathogens may alter their surface proteins to evade vaccine-induced immunity, as seen with certain strains of pneumococcus following the introduction of pneumococcal conjugate vaccines [64]. Monitoring these changes is crucial to ensure vaccines remain effective over time and to guide the development of next-generation vaccines.
The design of vaccines must carefully consider their impact on pathogen populations [65]. Overuse or improper deployment of vaccines can disrupt microbial ecosystems, potentially leading to unintended consequences, such as serotype replacement [66]. Therefore, balancing the scope of vaccine protection with a minimal ecological footprint is a key consideration in vaccine development and implementation.
5.3. Case Studies
The introduction of pneumococcal conjugate vaccines, such as PCV13, has significantly decreased the incidence of invasive pneumococcal diseases, including pneumonia, meningitis, and bacteremia [67]. In addition to improving public health, these vaccines have contributed to a notable decline in antibiotic use, as fewer bacterial infections necessitate treatment. PCV13 has shown effectiveness in reducing the prevalence of antibiotic-resistant strains of pneumococcus, showcasing how vaccines can complement antibiotic stewardship efforts [68, 69]. Despite the successes, challenges remain in fully leveraging vaccines to combat antibiotic resistance. Variability in vaccine access and coverage, particularly in low-resource settings, limits their impact on a global scale [70].
6. mRNA vs. DNA VACCINES: A PROMISING ALTERNATIVE FOR PNEUMONIA PREVENTION
mRNA vaccines have been recently used during the COVID-19 pandemic. Due to their quick development and induction of an immune response, they have been favored. A quick comparison of the mechanisms of DNA vaccines and RNA vaccines has been described below.
DNA vaccines typically consist of a circular plasmid containing inserted DNA that encodes an antigen. After injection, the plasmid must enter the host cell nucleus to be transcribed into mRNA, which is then exported to the cytoplasm and translated into the target antigen protein [71]. The expressed antigen is presented on antigen-presenting cells to elicit immune responses. Since DNA is more stable, these vaccines can often be stored at room temperature, and they have relatively low manufacturing costs and high stability compared to some traditional vaccines [72]. Figure 1 briefly explains, “How DNA Vaccines Work”. DNA incorporated into a vector, such as a plasmid, is introduced into the body using methods like electroporation, gene gun, lipid nanoparticles, or injection. The DNA enters body cells and goes to the nucleus. There, it is used to make proteins (antigens).
These antigens are presented to the immune system using MHC class I (expressed in all body cells) and II (expressed on antigen-presenting cells), which helps the body initiate an immune response [73].
mRNA vaccines contain a synthetic messenger RNA encoding the antigen of interest, typically delivered in a lipid nanoparticle for stability and cell entry. Once inside the host cell cytoplasm, the mRNA is directly translated by ribosomes to produce the antigen protein, which then triggers immune recognition [74]. Unlike DNA, the mRNA does not need to enter the nucleus or integrate into the genome, eliminating the risk of genomic integration [75].
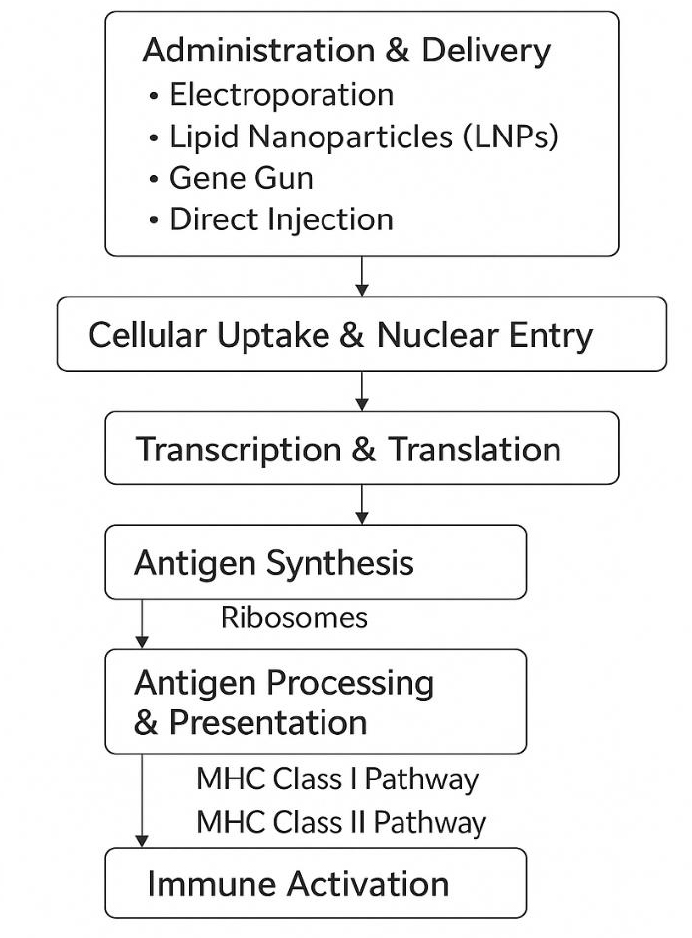
Schematic overview of the mechanism of DNA vaccines. After administration via methods like electroporation, lipid nanoparticles, gene gun, or direct injection, the DNA enters the cell and nucleus. It undergoes transcription and translation to produce antigenic proteins, which are then processed and presented through MHC class I and II pathways, leading to immune activation.
Available online under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecom mons.org/licenses/by/4.0/) [73].
The mRNA is inherently temporary; it is degraded after protein translation, which contributes to safety, but also demands efficient delivery to ensure sufficient protein is produced before degradation occurs. Both DNA and mRNA vaccines leverage the host cellular machinery to produce
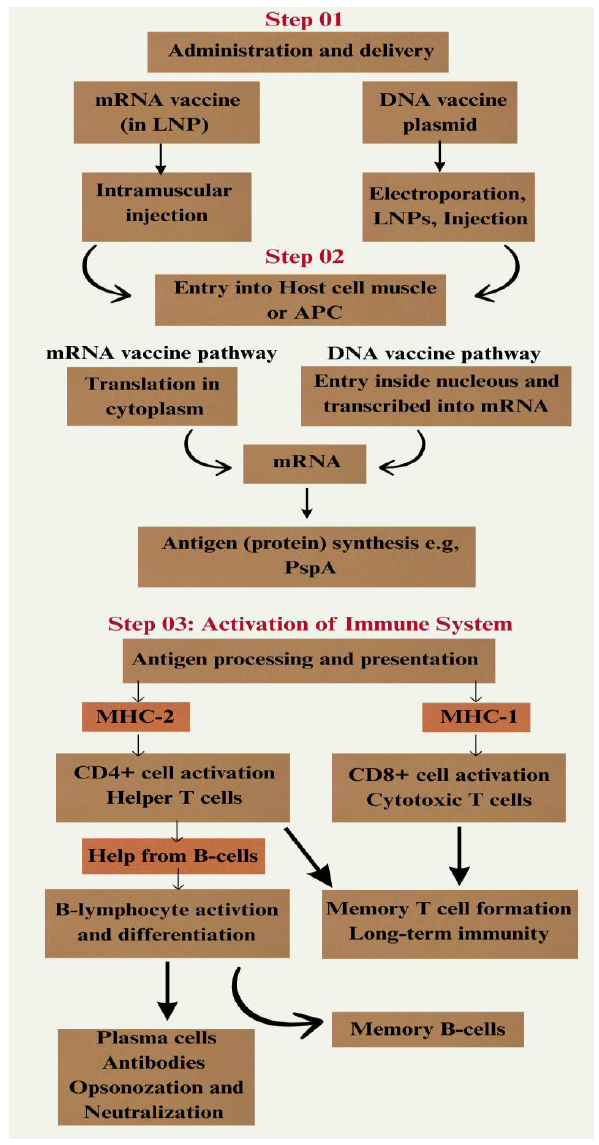
Comparative mechanism of action for mRNA and DNA vaccines.
Available online under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecom
mons.org/licenses/by/4.0/) [79, 80].
(Step 1): mRNA vaccines, formulated in lipid nanoparticles (LNPs), and DNA vaccines, part of a plasmid, are delivered through intramuscular injection or other methods like electroporation. After entry into a host cell (e.g., muscle cell or antigen-presenting cell) (Step 2), their pathways change. The mRNA is translated into the target antigen (protein) in the cytoplasm. The DNA plasmid construct enters the nucleus to be transcribed into mRNA, which then goes to the cytoplasm for translation. The synthesized antigenic proteins (e.g., PspA) are processed and presented on MHC I and MHC II molecules (Step 3). This antigenic presentation activates CD8+ cytotoxic T-cells and CD4+ helper T-cells, respectively. Helper T-cells help in activating B-cells, which differentiate into antibody-producing plasma cells and memory B-cells. This response generates antibodies for opsonization and neutralization, also memory cells for long-term immunity against pneumonia pathogens.
antigen in situ, eliciting both B-cell (antibody) and T-cell responses [76]. Notably, mRNA vaccines tend to activate innate immune sensors (e.g., endosomal Toll-like receptors and RIG-I/MDA5 in the cytosol) that can act as a natural adjuvant, whereas DNA plasmids may activate sensors like TLR9. The innate immune activation must be balanced; it can enhance adaptive responses, but if excessive, it can also cause inflammation. Advances, such as nucleoside modifications in mRNA (e.g., pseudouridine), have been used to reduce unwanted innate activation while maintaining immunogenicity [77, 78]. Though their intracellular delivery and processing requirements are different, the basic processes by which DNA and mRNA vaccines activate an immune response are the same in that they both use host cells to create antigenic proteins. Both platforms result in the presentation of antigens and the induction of a strong, diverse adaptive immune response, which includes both cellular and humoral immunity, essential for fighting pneumonia infections, as shown in Fig. (2) [79, 80].
6.1. mRNA Vaccines as a Promising Alternative, Especially for Pneumonia
The unparalleled success of mRNA vaccines in the past few years has reframed vaccine development. mRNA vaccines demonstrated “extraordinary performance” against COVID-19, with high efficacy and safety, encouraging researchers to expand this approach to many diseases. In comparison, DNA vaccines were largely overshadowed during the pandemic era [81]. The agility of mRNA technology – from rapid design to mass production – is a critical advantage when facing pneumonia-causing pathogens, which can emerge or mutate quickly. For instance, influenza viruses and coronaviruses can evolve new strains; an mRNA vaccine can be reprogrammed with a new sequence in a matter of weeks, whereas modifying traditional vaccine platforms can take months. This speed is pivotal for timely responses to outbreaks of respiratory infections [81, 82].
From an immunological perspective, mRNA vaccines also appear well-suited for combating pneumonia pathogens. They induce strong neutralizing antibody responses and robust T-cell responses, which are important for clearing respiratory infections. A notable benefit for respiratory viruses is that mRNA vaccines can be formulated as multivalent or combination vaccines. Since the manufacturing process is similar for any mRNA, it is feasible to combine multiple mRNAs in one formulation. This has opened the door to combination vaccines for respiratory infections – for example, clinical trials are underway for a combined mRNA vaccine targeting COVID-19, influenza, and RSV in a single shot. Such integrated approaches could be especially valuable for protecting vulnerable populations against the array of viruses that cause pneumonia [83, 84].
It is important to note that DNA vaccines are not being abandoned; they continue to be explored, and some experts argue that certain drawbacks of DNA vaccines (like delivery inefficiency) might be overcome with new techniques. Indeed, DNA vaccine research is ongoing for various infections. However, at present, the momentum is clearly behind mRNA platforms. The ability to avoid genomic integration risks while achieving equal or greater efficacy gives mRNA vaccines a distinct edge. A 2023 review succinctly stated that, compared to DNA vaccines, mRNA vaccines have a more favorable safety profile and allow “adjustable expression” of the antigen without lingering in the body. This makes them an attractive option for diseases like pneumonia, where safety is paramount (when vaccinating healthy populations) and where we may want immune responses that are strong but not chronically overstimulated [85, 86].
6.2. mRNA Vaccine Developments for Pneumonia-Causing Pathogens
Several mRNA vaccine candidates targeting pathogens that cause pneumonia are in development, with some already achieving clinical success. Respiratory Syncytial Virus (RSV) is a common cause of pneumonia in infants and older adults for which no vaccine existed until recently. An mRNA vaccine (Moderna’s mRNA-1345, brand name mRESVIA) encoding the RSV prefusion F protein was tested in a Phase 3 trial in older adults. It demonstrated 83.7% efficacy in preventing RSV-associated lower respiratory tract disease in adults over 60. In 2024–2025, this mRNA RSV vaccine gained regulatory approval for adults ≥60 and for high-risk adults aged 18–59, after showing robust protection with no significant safety concerns. This marks a major advance, as traditional vaccine approaches for RSV had failed for decades. The success of the RSV mRNA vaccine illustrates how mRNA technology can deliver effective vaccines against difficult respiratory viruses. Streptococcus pneumoniae (pneumococcus) is the leading cause of bacterial pneumonia and is responsible for hundreds of thousands of deaths annually [87]. Current pneumococcal vaccines are polysaccharide–protein conjugates covering multiple serotypes, but researchers are exploring mRNA approaches to target pneumococcal proteins common to all strains [88].
As of 2025, no pneumococcal mRNA vaccine has entered clinical trials, but the concept is actively being investigated. Experts note that the mRNA platform proven in COVID-19 could be “readily adapted” to pneumococcal antigens. Preclinical studies are likely underway to assess mRNA vaccines encoding conserved pneumococcal proteins (such as pneumolysin or PspA) in animal models. One challenge in pneumococcal pneumonia is that the bacteria often colonize the upper respiratory tract; thus, an effective vaccine may need to induce strong mucosal immunity (e.g., secretory IgA and tissue-resident T cells) to prevent colonization and infection [89]. Researchers are examining whether mRNA vaccines delivered intramuscularly can be optimized (or perhaps given via intranasal routes in the future) to generate mucosal protection as well [90]. If successful, an mRNA pneumococcal vaccine could provide serotype-independent protection by encoding conserved antigens, potentially overcoming the serotype replacement issues seen with current conjugate vaccines. Beyond RSV and pneumococcus, mRNA vaccine research extends to other pneumonia-related pathogens. Influenza, a major viral cause of pneumonia, is the target of several mRNA vaccine programs aiming to improve upon traditional flu shots; mRNA flu vaccines can be rapidly updated for new strains and have shown promising immunogenicity in early trials [91, 92]. Another important pathogen is Mycobacterium tuberculosis, the bacterium causing tuberculosis (TB), which often manifests as a chronic form of pneumonia. TB is the leading cause of infectious disease mortality globally (approximately 1.3 million deaths per year) [93]. Bacillus Calmette–Guérin (BCG) vaccine provides inconsistent protection in adults. Recent preclinical studies have shown that an mRNA vaccine against TB can elicit strong T-cell responses and enhance protection in animal models [94, 95]. In a 2025 mouse study, a lipid-nanoparticle mRNA vaccine induced immunity that significantly reduced TB bacterial load in the lungs, and it served as an effective booster after BCG vaccination. Researchers noted that this mRNA approach could be a “game-changer for bacterial diseases like TB,” given its rapid adaptability and potent immunogenicity. These findings are paving the way for future clinical trials in humans. The adaptability of mRNA technology also allows for combination vaccines [96]. Companies are testing combined respiratory vaccines (e.g., a single mRNA-based shot for COVID-19, influenza, and RSV) to simplify protection against multiple pneumonia-causing viruses.
Such innovations could significantly reduce the pneumonia burden, especially in older adults who are at risk from various pathogens [97].
7. INTEGRATED STRATEGIES TO PREVENT ANTIBIOTIC RESISTANCE
Integrating vaccines, antibiotics, and public health interventions is essential in combating infectious diseases and addressing antimicrobial resistance (AMR).
7.1. Use of Vaccines and Effective Delivery Systems
Vaccines play a pivotal role by preventing infections, thereby reducing the need for antibiotics and minimizing the emergence of resistant strains [98]. The World Health Organization (WHO) reports that vaccines against 23 pathogens could decrease global antibiotic use by 22%, equating to 2.5 billion defined daily doses annually [99]. Increasing funding and collaboration for vaccine research, particularly in relation to pneumonia, has now become an urgent area for global health consideration due to the persistent and deadly burden of this disease, particularly in children in developing regions. Pneumonia is responsible for the death of over two million children under the age of five every year worldwide; the great majority of these deaths occur in resource-poor countries, where therapeutic access remains low and vaccination coverage is inadequate [100]. The development and eventual delivery of effective vaccines, therefore, require not only scientific innovation but also strategic financial mechanisms and global partnerships to make it happen. One such strategy is the Advanced Market Commitment (AMC), which provides pharmaceutical companies with an incentive to pursue late-stage development by guaranteeing a market and subsidizing part of the cost of production for low-income countries. This innovative financial mechanism guarantees that manufacturers could sell the vaccines at an affordable price, bridging the commercial viability and public health need gap [101].
Public health interventions, such as improved sanitation, hygiene, and surveillance, complement vaccination efforts by controlling the spread of infections and ensuring the rational use of antibiotics. This integrated approach not only enhances disease prevention but also preserves the efficacy of existing antibiotics [102].
7.2. Rational Antibiotic Use
Encouraging rational antibiotic use alongside vaccine deployment is crucial to prevent the overuse and misuse of antibiotics, which are primary drivers of AMR. Implementing antimicrobial stewardship programs that promote appropriate prescribing practices, along with widespread vaccination, can substantially reduce unnecessary antibiotic consumption. The WHO underscores that vaccines can decrease the incidence of infections, thereby reducing the need for antibiotics and the subsequent development of resistance [103].
Despite these advances, however, challenges remain, such as the criticism of the AMC for being inflexible and detrimental to the adoption of other new, potentially better vaccines during its limited operational period. Besides, the risk of pneumonia is further aggravated by the presence of HIV, with children infected with HIV showing a 40 times higher propensity towards invasive pneumococcal diseases than uninfected peers. Clinical observations from South Africa and other excessively burdened areas indicated that more than 50% of children admitted due to pneumonia are HIV positive; this is a good reason to develop vaccines for immunocompromised populations [104]. Moreover, pneumonia pathogens, Streptococcus pneumoniae and Haemophilus influenzae type b, underscore the need for comprehensive vaccine coverage and multivalent formulations [105].
7.3. Global Efforts and Policy Recommendations: Strengthening Global Surveillance for Antibiotic Resistance
Antimicrobial resistance (AMR) poses a significant threat to global health, necessitating robust surveillance systems to monitor and combat resistant infections. The World Health Organization (WHO) has established the Global Antimicrobial Resistance and Use Surveillance System (GLASS) to provide standardized data on AMR patterns worldwide. This initiative aims to enhance the quality, quantity, and sharing of data on AMR, thereby informing national and international policies and strategies [106].
7.4. Policy Recommendations
To enhance global surveillance and scale down the impact of AMR in pneumonia, the following policy measures are recommended:
7.4.1. Expand GLASS Participation and Data Quality
Encourage universal enrollment and active participation of all WHO member states in GLASS. Countries should be supported in establishing sentinel surveillance sites for pneumonia and adopting standardized laboratory protocols [107].
7.4.2. Invest in Laboratory Infrastructure and Workforce
Strengthen national laboratory networks with sustained investments in diagnostic equipment, data systems, and workforce training. Further, national reference laboratories and regional centers of excellence should be established for pneumonia pathogen testing [108].
7.4.3. Integrate Genomic Surveillance
Scale up the adoption of WGS technologies for high-priority pneumonia pathogens. Create interoperable databases that link genomic, clinical, and epidemiological data for real-time decision-making [109].
7.4.4. Promote One Health Collaboration
Foster cross-sectoral coordination between human, veterinary, and environmental health sectors. Surveillance of respiratory pathogens in animals and environmental samples should be included to understand the full scope of resistance transmission [110].
7.4.5. Leverage Vaccination Programs
Integrate AMR surveillance with vaccination coverage monitoring. Evaluate the Outcome of pneumococcal conjugate vaccines (PCVs) on resistance trends and serotype replacement. Additionally, vaccine-driven reductions in pneumonia incidence should be used to optimize antibiotic stewardship [111].
7.4.6. Ensure Data Transparency and Global Data Sharing
Promote open access to AMR surveillance data while ensuring ethical standards and data security. Data-sharing platforms should support interoperability across countries and institutions [112].
7.4.7. Incorporate Surveillance Findings into Treatment Guidelines
Use real-time resistance data to update national and international clinical guidelines for pneumonia management. Incorporating local AMR trends ensures the rational and effective use of antibiotics [113].
7.5. Increasing Funding and Collaboration for Vaccine Research
Advancing vaccine research is crucial for preventing infectious diseases and preparing for future pandemics. Collaborative efforts among governments, international organizations, and private entities are crucial to accelerate vaccine development and distribution. For instance, the Sabin Vaccine Institute emphasizes the importance of social and behavioral research grants to support immunization policies and programs, highlighting the need for increased funding and collaboration in vaccine research [114]. The AMC program for pneumococcal vaccines, primarily financed by major patrons, such as Canada, Italy, Norway, the Russian Federation, the United Kingdom, and the Bill & Melinda Gates Foundation, has committed $1.5 billion to secure vaccine availability and affordability to prevent five million deaths by 2030. Strong delivery systems, coupled with diagnostics and healthcare capabilities, are essential components in vaccination programs, especially for higher-risk immunocompromised infants. This is where the public-private partnership of the GAVI Alliance becomes crucial in reaching the neglected populations and sustaining immunization programs. Funding, innovating, and having readiness for flexible approaches will work in favor of further reduction of child mortality from pneumonia [104].
8. CHALLENGES AND LIMITATIONS OF NOVEL VACCINE PLATFORMS
Despite their significant promise, both DNA and mRNA vaccine platforms face considerable challenges that must be overcome for their widespread application against pneumonia and other diseases.
8.1. DNA Vaccine-specific Challenges
The main problem with DNA vaccines has been their weak ability to provoke strong immune responses in human trials compared to animal models. This often necessitates high doses or repeated administrations, which is impractical for large-scale vaccination campaigns [73]. There is also a theoretical (but very low) risk that plasmid DNA could integrate into the host genome and alter host DNA, raising concerns about insertional mutagenesis or autoimmunity [115].
The need for the DNA plasmid to cross both the cell and nuclear membranes creates a delivery barrier, limiting transfection efficiency and antigen expression.
Most DNA vaccine plasmids contain antibiotic resistance genes as selectable markers during the manufacturing process. There is a theoretical concern about the horizontal transfer of these genes to gut microbiota or environmental bacteria, potentially contributing to antimicrobial resistance (AMR) [116].
In some cases, the prolonged, low-level antigen expression from DNA vaccines has been associated with the induction of immune tolerance rather than protective immunity, particularly for certain antigens [106].
8.2. mRNA Vaccine-Specific Challenges
mRNA vaccines, especially those using certain lipid nanoparticles (LNPs), can be associated with significant local and systemic reactogenicity, including fever, fatigue, and myalgia. While generally transient, this can impact vaccine acceptance and poses a challenge for use in vulnerable populations [39]. Despite improvements, mRNA is inherently less stable than DNA and typically requires storage at ultra-low temperatures (-20°C to -80°C) to maintain efficacy. This poses a major challenge for distribution in low-resource settings, where the burden of pneumonia is highest [84].
As a newer technology, long-term data on the durability of immune protection and the infrequent adverse events for mRNA vaccines are still being collected for various disease targets beyond COVID-19.
8.3. Platform-agnostic Challenges
While promising, scaling up the manufacturing of complex formulations like LNPs for global supply remains a challenge [117]. The cost of goods for these novel vaccines is currently higher than for many traditional vaccines [118]. Public skepticism towards new genetic-based vaccine technologies remains a significant hurdle. Clear communication and transparency about the development, safety, and mechanisms of these vaccines are crucial for public acceptance. As with all vaccines, there is a constant evolutionary arms race. Therefore, continuous surveillance and platform agility are required to address this issue [119].
CONCLUSION
This review highlights that both DNA and mRNA vaccine technologies represent hopeful strategies for fighting pneumonia. DNA vaccines offer stability and cost-effectiveness but face challenges in achieving strong immunogenicity, which could be solved through better adjuvants and delivery systems. mRNA vaccines, on the other hand, have shown success against respiratory viruses, with the current approval of an mRNA vaccine for RSV indicating their possibility for pneumonia prevention and for producing multivalent vaccines against multiple pathogens. Constant investment in nucleic acid vaccine research is important, as both platforms could significantly reduce the burden of pneumonia and the associated selective pressure causing antibiotic resistance. Future work should focus on improving DNA vaccine delivery and expanding mRNA applications to bacterial and viral pathogens, thereby confirming their inclusion in global public health strategies.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: M.A.: Study conception and design; M.A., H.H., and M.M.: Data collection; Z.N. and A.S.: Analysis and interpretation of results; R.: Data curation; H.K., S.S.A., and Q.K.: Writing - reviewing and editing; S.E.: Writing the paper; R.A.: Investigation; M.A.: Conceptualization. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AMC | = Advanced Market Commitment AMR Antimicrobial Resistance APCs Antigen-Presenting Cells |
| BCG | = Bacillus Calmette-Guérin (vaccine) CPS Capsule Polysaccharides |
| CpG ODNs | = CpG Oligodeoxynucleotides |
| DNA | = Deoxyribonucleic Acid |
| GLASS | = Global Antimicrobial Resistance and Use Surveillance System |
| GM-CSF | = Granulocyte-Macrophage Colony-Stimulating Factor |
| IL-23 | = Interleukin-23 |
| LNPs | = Lipid Nanoparticles |
| MDR | = Multidrug-Resistant |
| PAMPs | = Pathogen-Associated Molecular Patterns PCVs Pneumococcal Conjugate Vaccines |
| PPSV23 | = Pneumococcal Polysaccharide Vaccine (23-valent) |
| PS | = Polysaccharide |
| PsaA | = Pneumococcal Surface Adhesin A |
| PspA | = Pneumococcal Surface Protein A |
| RSV | = Respiratory Syncytial Virus |
| TB | = Tuberculosis |
| TLR | = Toll-Like Receptor |
| WHO | = World Health Organization |
| mRNA | = Messenger Ribonucleic Acid |
ACKNOWLEDGEMENTS
Declared none.
DECLARATION OF GENERATIVE AI AND AI-ASSISTED TECHNOLOGIES IN THE WRITING PROCESS
The authors acknowledge the use of ChatGPT (OpenAI) in the initial drafting and refinement of the manuscript. ChatGPT was utilized for language enhancement, summarizing relevant literature, and improving clarity. All content generated by AI was critically reviewed, validated, and revised by the authors to ensure accuracy, originality, and compliance with academic standards.

