All published articles of this journal are available on ScienceDirect.

Emergence of Highly Pathogenic Avian Influenza H5N1 Virus in Humans
Authors Info & Affiliations
Editorial
Although avian influenza A viruses are highly species-specific, they can occasionally cross the species barrier to infect other species and cause highly lethal disease. In 1997, 18 human cases of H5N1 avian influenza were first reported in Hong Kong. A new outbreak occurred in 2003. Since then, the HPAI H5N1 virus has evolved rapidly. On 26 February 2024, WHO reported the first five laboratory-confirmed human cases in Cambodia, including one death. Since 2003, the new HPAI H5N1 viruses have killed 466 people out of 964 cases. To cause a pandemic, the virus must be antigenically novel, virulent, and transmissible between humans. A pathogen that lacks at least one of these characteristics has the potential to cause a pandemic. Currently, H5 viruses do not have the potential to cause a pandemic because they cannot yet be transmitted from person to person. However, it may take very little time for H5 viruses to acquire pandemic potential. The purpose of this editorial was to express the opinion of the authors on such an important topic given the spread of the avian flu virus around the world. Unfortunately, the COVID-19 pandemic demonstrated our unpreparedness for global disasters. Hence, we should learn lessons from it. At the onset of the 2009 influenza pandemic, WHO considered scaling up the production of live-attenuated influenza vaccine (LAIV) as a promising strategy in a pandemic situation. Unlike inactivated vaccines, LAIVs are capable of inducing broad and long-term immune responses, making them an attractive option for pandemic preparedness, particularly in countries with very high population densities. Global surveillance and pre-pandemic preparedness for defense against H5N1 influenza viruses are public health concerns, which warrant intensive development of potential pandemic vaccines, including LAIV.
1. INTRODUCTION
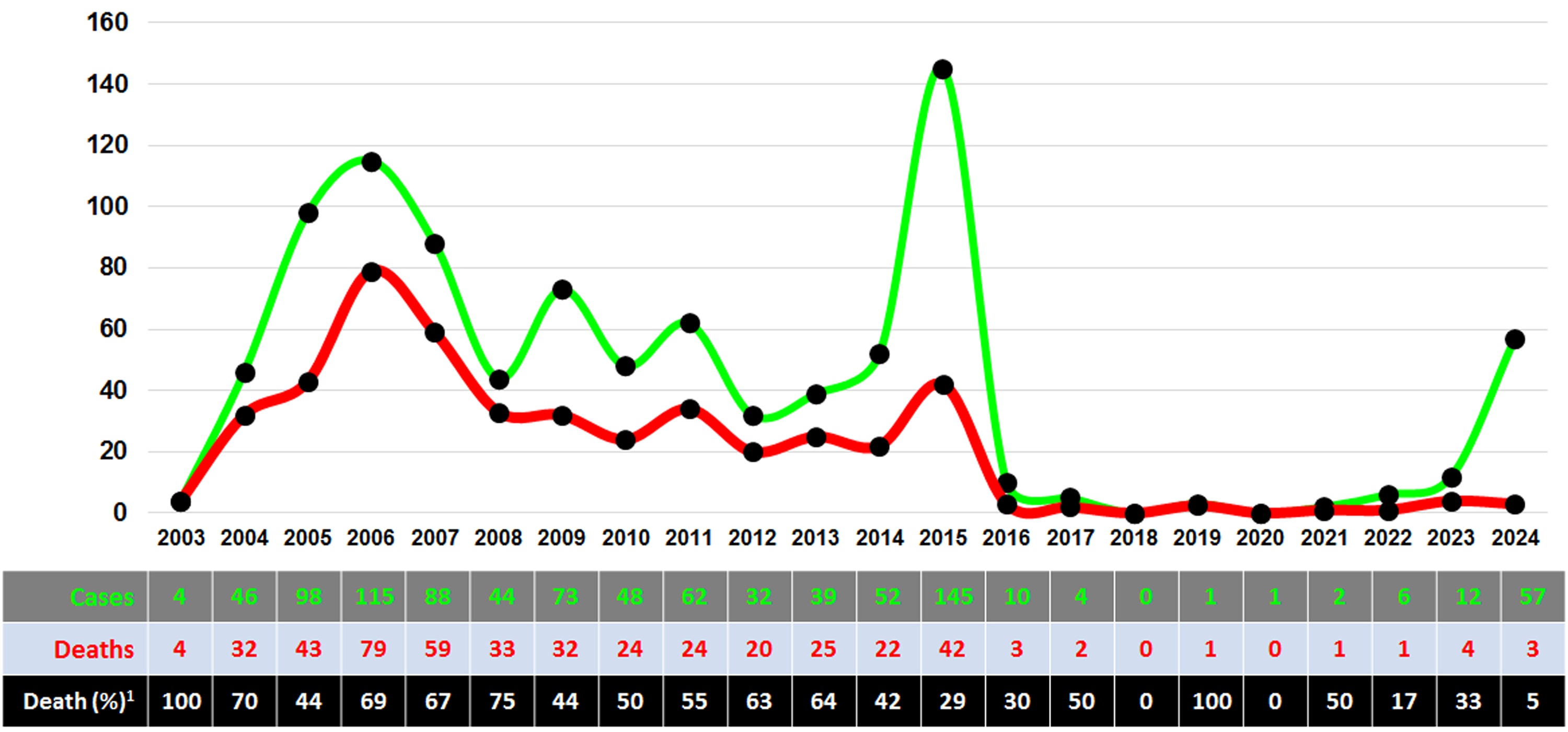
Although avian influenza A viruses are highly species-specific, they can occasionally cross the species barrier to infect other species and cause a highly lethal disease. In 1997, 18 human cases of H5N1 avian influenza were first reported in Hong Kong. Six of them (33%) were fatal [1, 2]. The outbreak was brought under control after a large number of birds were eliminated. A new outbreak occurred in 2003. Since then, the highly pathogenic avian influenza H5N1 virus (HPAIV) has evolved rapidly (Fig. 1). Circulating H5N1 viruses are classified into 10 clades and subdivided into numerous subclades, which frequently undergo reassortment [3, 4]. To date, the most divergent clade 2 consists of 39 subclades with different antigenic characteristics [5, 6]. Of greatest concern are cases of HPAIV, which is transmissible to humans, resulting in severe respiratory infections and high mortality.
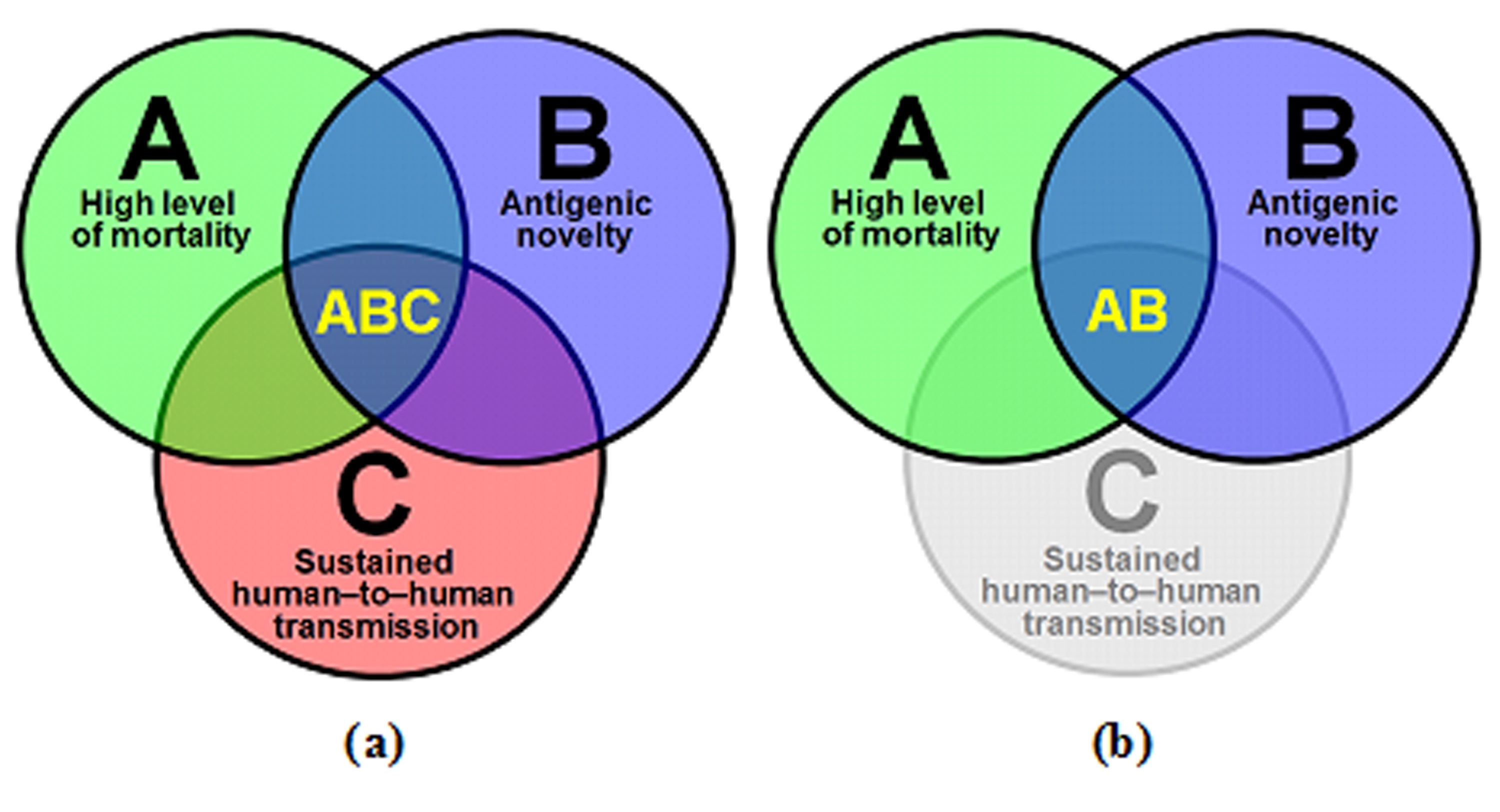
Euler circle diagram: correlations between pandemic (a) and potential pandemic (b) virus characteristics: A - high mortality, B - antigenic novelty, and C - sustained human-to-human transmission.
Since 2017, human cases of H5N1 have become rare and sporadic events, and the evolution of H5N1 viruses has not dramatically increased the risk to public health (Fig. 1). However, on February 26, 2024, five laboratory-confirmed human cases in Cambodia, including one death, were reported by WHO [7]. On March 28, 2024, there were already 6 cases (2 deaths) reported, 7 (2 deaths) on May 3, 2024; 11 (2 deaths) on June 7, 2024; 14 (2 deaths) on July 19, 2024; 22 (3 deaths) on September 27, 2024; and 57 (3 deaths) on November 1, 2024. The latest available information was provided on December 12, 2024; a total of 72 laboratory-confirmed cases of human infection with the H5N1 avian influenza virus, including 3 deaths, have been reported worldwide (the vast majority of cases have been reported in Cambodia, i.e., 10, and the United States, i.e., 58) [7]. From December 2003 to December 2024, the HPAI H5N1 virus killed 464 people out of 954 laboratory-confirmed cases, as reported by WHO (49.4%) [7].
Of serious concern is the fact that the currently circulating H5N1 virus causes not only a typical respiratory illness, but also conjunctivitis [9]. It has been detected in dairy herds [10-12], wastewater [10], and on the surfaces of milking machines [13]. Also, it has been isolated from unpasteurized milk [13]. The above facts, as well as the widespread invasion of the virus in Cambodia and several American states, raise concerns regarding the potential danger to human health posed by the H5N1 virus.
To date, the viruses of subclades 2.3.2.1 (a-g) and 2.3.4.4 (a-h) are of greatest concern with respect to pandemic threat; these variants predominate in animals, and recent human isolates have been subtyped as 2.3.2.1с and 2.3.4.4b variants [14]. Human infections with subclade 2.3 viruses in 2005-2006 were associated with increased mortality [15]. Of particular concern is the discovery of reassortants between these two subclades, one of which was isolated from a fatal human case in Cambodia in September 2024 [16]. An analysis of the amino acid alignment of polymerase complex proteins of 2023-2024 human isolates showed that in the list of 2.3.2.1с and some 2.3.4.4b isolates were detected amino acid substitutions that were characterized as associated with increased virulence in mammals, including PB2 E627K, PB2 D701N, and PB1 S375N [17]. A severe case was detected in November 2024 in British Columbia, Canada [18]. The possibility of direct HPAI H5N1 virus entry from wild bird populations, together with the high likelihood of reassortment and ubiquitous distribution of 2.3.4.4b viruses in different animal species, increases the risk of a pandemic threat.
The WHO has identified 17 top high-risk pathogens for vaccine development [19, 20], stating that a high risk of a public health emergency of international concern has been identified in the form of H5 viruses in 2024 [20], which calls for increased global surveillance for avian influenza in animals (wild birds, swine, dairy cattle) [21].
For a pathogen to cause a pandemic, it should be (i) antigenically novel to the human immune system, (ii) virulent, and (iii) human-to-human transmissible and ubiquitous in the human host [22]. In Fig. (2a), the factors that make a pathogen gain the potential to cause a pandemic are shown in the form of an Euler diagram (Euler circles). A strain missing at least one of the circles is potentially pandemic-causing (Fig. 2b).
As shown in Fig. 2b, it takes very little time for a pathogen to acquire pandemic potential. In the case of H5N1 influenza viruses, there is an absence of sustained human-to-human transmission. H5N1 viruses are characterized by high lethality and novelty to the human host, but they are not very efficient at human-to-human transmission. Sensational experiments by Ron A. M. Fouchier [23] confirmed that by targeted mutagenesis and passages through ferrets, it is possible to obtain an H5N1 virus capable of uncontrolled spread among mammals, that is, restoring the third circle in Euler's diagram.
To date, nature has almost brought these innovative experiments to life. Now, it can happen in real life as well. Once everyone was sure that the next pandemic would be caused by the H5N1 bird flu virus; however, instead of this, in 2009, the H1N1pdm09 swine flu virus appeared [24]. What we can be sure of is that there will be a next pandemic. Only time will tell us which pathogen will cause it. In drawing lessons from the 2009 pandemic, it is worth recalling that at the beginning of the pandemic, WHO considered the expansion of live attenuated influenza vaccine (LAIV) production as a promising strategy to increase the supply of influenza vaccines in a pandemic situation [25]. Unlike inactivated vaccines, LAIVs can provide a first line of defense by inducing broad and long-lasting immune responses, which makes them an attractive option for pandemic preparedness, particularly in countries with very high population densities.
CONCLUSION
In January 2025, a new fatal case occurred in Cambodia, bringing the global count to a total of 964 cases and 466 deaths caused by the H5N1 virus [26]. This indicates that the risk of an H5N1 pandemic remains. Global surveillance and pandemic preparedness for H5N1 influenza viruses are public health concerns, which warrant intensive development of potential live and inactivated pandemic vaccines.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: data collection: E.B.; analysis and interpretation of results: E.S.; drafting of the manuscript: I.K. All authors have reviewed the results and approved the final version of the manuscript.
ABBREVIATION
| LAIV | = Live Attenuated Influenza Vaccine |
FUNDING
The manuscript was funded by the budget provided by the IEM, Russia (code: FGWG-2025-0015) and received no external funding.
CONFLICT OF INTEREST
Dr. Irina Kiseleva is the Editor in Chief of the journal The Open Microbiology Journal.
ACKNOWLEDGEMENTS
Declared none.

