All published articles of this journal are available on ScienceDirect.

Molecular Identification and Characterization of the Causative Species of Cutaneous Leishmaniasis in Dezful City, Southwest Iran
Authors Info & Affiliations
Abstract
Background
Cutaneous Leishmaniasis (CL) represents a significant public health concern in endemic regions such as Dezful City, Iran, where cases have recently surged. This study aimed to identify and characterize the molecular profile of CL-causing species among patients in Dezful.
Methods
A total of 94 patients with skin lesions were enrolled, and demographic data, including age, gender, and residency, were collected. For each patient, two smears were obtained from the lesions: one for microscopic diagnosis and the other for DNA extraction. Subsequent molecular identification of the parasite was performed using Polymerase Chain Reaction (PCR). PCR amplification targeted the ITS1 region using specific primers Leish R (5’-AAA CAA AGG TTG TCG GGG-3’) and Leish F (5’-CAA CAC GCC GCC TCC TCT CT-3’).
Results
The results revealed that 100% of the CL cases were attributed to Leishmania major (L. major). Among the 94 patients, 67 (71.3%) were male, while 27 (28.7%) were female, with the highest incidence occurring in the age group of 11 to 20 years. Notably, lesions predominantly affected the hands (38.3%), whereas simultaneous involvement of the hand and trunk was present in only two cases (2.1%). Of the patients examined, 27 (28.7%) presented with a single lesion, 32 cases (34%) with two, 20 cases (21.3%) with three, and 15 (16%) with four or more lesions. Most of the lesions were observed to have a duration of one month (50%).
Conclusion
This study underscores the predominance of L. major in CL cases in Dezful, highlighting its epidemiological significance and the need for ongoing surveillance and control measures in the region, particularly focusing on controlling reservoirs (wild rodents).
1. INTRODUCTION
Cutaneous Leishmaniasis (CL) is a significant public health concern caused by parasitic protozoa belonging to the genus Leishmania, which are transmitted to humans through the bites of infected phlebotomine sandflies [1]. The lifecycle of these parasitic protozoa is digenetic. It begins with the presence of flagella, where the parasites enter a promastigote phase within the sandfly vector. Once the parasites infect a mammalian host, they transition to an aflagellate amastigote stage [2]. According to various reports, around twelve million individuals in 100 countries are impacted by this skin infection, and approximately 350 million people are at risk [3-6]. According to the World Health Organization, the annual number of new cases is estimated at 1,500,000 [7]. Over 90% of CL cases occur in Afghanistan, Algeria, Saudi Arabia, Iran, Syria, Bolivia, Brazil, Colombia, Nicaragua, and Peru [4]. Leishmaniasis is present in 14 out of 22 countries in the Middle East region, meaning that CL has become a significant health problem in more than two-thirds of these countries. In Iran, the disease has been steadily increasing, and it is endemic in 17 provinces [8]. The World Health Organization recognizes this condition as one of the most critical parasitic diseases worldwide (4-5). Leishmaniasis ranks among the top three diseases identified by the World Tropical Diseases Research Center, alongside African trypanosomiasis and dengue fever [9, 10]. The disease is characterized by a range of manifestations, from manageable skin ulcers to severe visceral forms [11, 12]. In tropical areas, the likelihood of disease transmission to humans is influenced not only by environmental elements like vegetation and climate but also by the socioeconomic traits of the local populations. Nevertheless, the extent to which these factors affect the risk and occurrence of disease remains unclear [13]. In Iran, two species of Leishmania, L. tropica and L. major, are responsible for anthroponotic and zoonotic CL, respectively [14]. Phlebotomus papatasi is recognized as the vector, and Tatera indica and Nesokia indica are identified as reservoirs for this disease in Iran, particularly in Dezful County [15]. The most important control measures to reduce the incidence of the disease include wearing appropriate clothing to prevent bites from sand flies, the vectors of the disease, especially in rural areas. Additionally, active case finding and prompt treatment of infected individuals are key strategies to interrupt the transmission cycle of the disease [16, 17]. Pathologically, CL lesions typically manifest as an erythematous papule, which then progresses to a macule and may subsequently develop into a nodule and ulcer, eventually healing with a scar [18]. The incubation period for rural CL, caused by Leishmania major, ranges from several weeks to several months. After this period, the lesion appears as a pimple with acute inflammation. Ulceration occurs within 10 to 14 days after the appearance of the pimple [19]. Diagnosis is based on parasitological methods, involving sampling of the lesion margin and microscopic examination of the samples to identify the parasite as intracellular or extracellular Leishman bodies [18]. Despite advancements in research and the introduction of new therapeutic agents for the effective treatment of CL, pentavalent antimony compounds, such as glucantime, continue to be the first-line treatment for this disease [20]. In the past few decades, there have been instances of new leishmaniasis foci emerging or expanding in Iran, reflecting shifts in the epidemiology of the disease. Notably, these areas have now become endemic [21, 22]. Key factors contributing to this trend include alterations in environmental conditions, such as climate change, as well as human influences, like travel to endemic regions and migration [23].
Khuzestan Province is one of the key endemic areas for CL in Iran. Within this province, Dezful City stands out as a major focus of the disease. Historically, these areas were relatively limited; however, factors such as population growth, the influx of non-immune, non-Iranian populations, and the expansion of residential developments near the habitats of disease-carrying rodents have contributed to the emergence and changing patterns of CL in this region. Consequently, the disease has become a significant public health issue in Dezful County. The number of reported cases has sharply increased from 372 new cases in 2013 to 1,917 cases by 2015, highlighting it as a critical area of concern [24]. This underlines a shift from a low-incidence area to a re-emerging focus of CL, influenced by its geographical proximity to endemic regions in Iraq and other Iranian provinces [25]. In Dezful, a city known for its diverse ecological zones and climate, the occurrence of CL presents a unique challenge that necessitates the implementation of molecular techniques for the identification and genotyping of Leishmania species [26]. The accurate identification of Leishmania species is crucial for effective disease management, as traditional diagnostic approaches often lack the necessary sensitivity and specificity. Molecular techniques, particularly Polymerase Chain Reaction (PCR), have emerged as powerful tools for the molecular characterization of Leishmania species, enabling precise identification of strains and monitoring of their genetic diversity [27]. An increased understanding of the molecular epidemiology of CL can assist in developing targeted interventions and fostering the effective management of this neglected tropical disease. Given the observed behavioral changes in Leishmania parasites, reports of relapses and drug resistance, as well as the emergence of varied and atypical skin lesions in CL patients in Dezful County, the likelihood of the introduction of different Leishmania strains has significantly increased. This study was conducted with the aim of molecular identification of CL in Dezful city, southwestern Iran, which will contribute critical data for a broader understanding of this disease in the region and provide insights for successful public health strategies.
2. METHODS
2.1. Study Design
A flowchart was designed for this study, and the research steps were carried out in order (Fig. 1).
2.2. Study Area
This study was conducted in Dezful, located in the Khuzestan Province of Iran, along the Dez River, nestled within the Central Zagros Mountains. Dezful is a city rich in history and cultural significance. The geographical coordinates of Dezful position it approximately 32.4°N latitude and 48.4°E longitude, giving it a unique climate that features hot summers and mild winters, characteristic of the southwest Iranian plateau. Geographically, it is bordered by Andimeshk and Aligoodarz Counties to the north, Lali District of Masjed Soleiman City to the east, and Shush City to the south and west [28].
2.3. Sampling and Patient Selection
A total of 94 Giemsa-stained smears were collected from patients (male and female) of different age groups at the leishmaniasis Reference Laboratory in Dezful City during 2022 - 2023. These samples were subsequently sent to the central laboratory of Dezful University of Medical Sciences, Khuzestan, Iran, for analysis. The demographic data, including age, sex, residence, number of lesions, and duration of lesions, were documented using standardized questionnaires. Diagnosis of leishmaniasis was based on the microscopic detection of amastigotes, which were observed from lesion exudates prepared as smears, fixed in methanol, and stained with Giemsa for light microscopy examination. The scoring for parasitic density was conducted following WHO classification guidelines, ranging from 4+ (1–10 parasites/field) to 1+ (1–10 parasites/1000 fields) [29].
2.4. DNA Extraction and PCR Amplification
Genomic DNA was extracted from 94 selected samples using a commercial DNA extraction kit (Sinaclon, Iran), following the manufacturer’s instructions. To evaluate the extracted DNA's quantity and quality, we measured the concentration with a NanoDrop UV-Vis spectrophotometer and performed electrophoresis on a 1% agarose gel [30]. The extracted DNA was preserved at -20°C until further utilization. PCR amplification targeted the ITS1 region using specific primers Leish R (5’-AAA CAA AGG TTG TCG GGG-3’) and Leish F (5’-CAA CAC GCC GCC TCC TCT CT-3’). The reaction mixture included 7.5 µL of PCR master mix, 4 µL of distilled water, 0/75 µL of each primer, and 2 µL of sample DNA, reaching a final volume of 15 µL. The cycling conditions involved an initial denaturation step at 95°C for 5 minutes, followed by 35 cycles of denaturation at 95°C for 30 seconds, annealing at 60°C for 30 seconds, and extension at 72°C for 30 seconds, concluding with a final extension at 72°C for 3 minutes. The amplified fragments of L. infantum were 603 bp in length, while the fragments of L. tropica and L. major measured 520 bp and 670 bp, respectively, which was visualized on 1% agarose gels stained with a safe staining agent under UV light.
2.5. Ethical Considerations
This study was conducted following the ethical guidelines approved by the Ethics Committee of Dezful University of Medical Sciences, Khuzestan, Iran (IR.DUMS.REC.1401.060). Informed oral consent was obtained from all participants, ensuring confidentiality and anonymity of patient information in line with ethical research practices.
2.6. Statistical Analysis
The collected data were analyzed in SPSS (version 16). Quantitative data were reported through mean and standard deviation and qualitative data were reported by percentage. Collected data were analyzed using appropriate statistical methods, including Fisher's exact test and chi-square test, to determine associations between demographic factors and the prevalence of different Leishmania species. Statistical significance was set at a p-value of <0.05.
3. RESULTS
In this investigation, we analyzed 94 patients diagnosed with CL through microscopy at a magnification of 1000×. In this study, the age distribution of participants was as follows: < 10 years: 8 patients (8.5%), 11-20 years: 30 patients (31.9%), 21-30 years: 19 patients (20.2%), 31-40 years: 15 patients (16.0%), and > 40 years: 22 patients (23.4%). The highest frequency of cases infected with CL according to age was found in the age group of 11 to 20 years, and the lowest frequency in the age group of less than 10 years. Among these subjects, the gender distribution was 67 males (71.3%) and 27 females (28.7%), indicating a higher prevalence among males. The distribution of wounds based on the location of the lesion was as follows: 36 patients (38.3%) on the hand, 26 patients (27.7%) on the foot, 15 patients (16%) on the face, and 17 patients (18.0%) on other parts of the body. Most of the lesions (38.3%) were on the hands, and 34.0% of the patients had two lesions. The direct smear examination yielded varying levels of parasitemia [1+ with 24 cases (25.5%), 2+ with 24 cases (25.5%), 3+ with 31 cases (33%), and 4+ with 15 cases (16%)], exhibiting a parasitemia level of 4+ (Table 1).
In this study, the distribution of lesion duration among the 94 patients diagnosed with CL revealed that 50% of the patients had lesions persisting for one month. In contrast, 27.7% had lesions lasting less than one month, and 19.1% had lesions lasting two months or more. The remaining cases had lesion durations of three months or longer, with only a small percentage exhibiting very prolonged lesions (2.1%). In terms of the duration of the ulcer in 47 cases (50%), it was one month (Table 1).
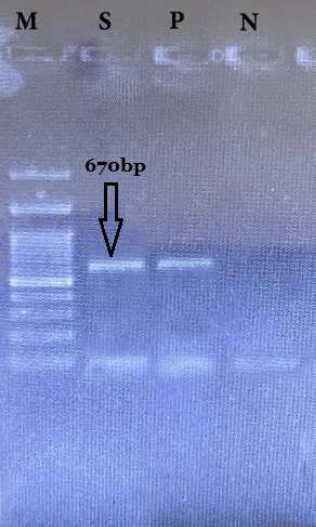
Further molecular analysis using PCR detected Leishmania spp. in 94 clinical samples, confirming the presence of the pathogen, of which 94 cases (100%) were L. major and 0 cases (0%) were L. tropica (Table 1). PCR amplification of ITS1 in 94 clinical samples yielded fragments of about 670 bp. (Fig. 2).
| Characteristic | N (%) |
|---|---|
| Age groups (year) | |
| < 10 | 8 (8.5%) |
| 11-20 | 30 (31/9%) |
| 21-30 | 19 (20.2%) |
| 31-40 | 15 (16.0%) |
| > 40 | 22 (23.4%) |
| Gender | |
| Female | 27 (28.7%) |
| Male | 67 (71.3%) |
| Location of lesion | |
| Hand | 36 (38.3%) |
| Leg | 26 (27.7%) |
| Face | 15 (16%) |
| Other parts the body | 17 (18.0%) |
| Number of lesions | |
| 1 | 27 (28/7%) |
| 2 | 32 (34/0%) |
| 3 | 20 (21/3%) |
| > 3 | 15 (16/0%) |
| Wound period | |
| < 1 | 26 (27.7%) |
| 1 month | 47 (50%) |
| 2 months | 18 (19.1%) |
| 3 months | 1 (1.1%) |
| > 3 | 2 (2.1%) |
| Parasitemia rate | |
| +1 | 24 (25.5%) |
| +2 | 24 (25.5%) |
| +3 | 31 (33%) |
| +4 | 15 (16%) |
| Parasite species | |
| L. major | 94 (100%) |
| L. tropica | 0 (0%) |
4. DISCUSSION
The findings of this study highlight the critical public health issue posed by CL in Dezful City, Iran, identifying L. major as the sole causative agent among the sampled population. This aligns with previously established literature that indicates L. major as a predominant species responsible for zoonotic CL in various regions of Iran [14, 21]. The increase in CL incidence in Dezful warrants attention due to its geographical proximity to endemic areas and the implications for local health systems in managing the disease. Hadad et al. conducted a study from 2012 to 2013 to identify the causative species of CL in Mehran County, Ilam Province. Their findings revealed that 100% of the identified species were L. major, which is consistent with our own results [9]. The dominance of L. major can be explained by the geographical proximity of Khuzestan and Ilam provinces, as well as the presence of shared reservoirs and vectors.
The demographic analysis revealed a striking gender imbalance, with males accounting for approximately 71.3% of cases. This aligns with trends observed in other studies, suggesting a higher exposure risk among males, possibly due to their involvement in outdoor activities [10, 23]. The most affected age group was identified as 11 to 20 years, which may indicate that younger individuals are more susceptible, potentially due to increased outdoor exposure or occupational hazards typical in endemic areas [4, 28].
Lesion localization predominantly on the hands (38.3%) raises important considerations for the social and psychological impact on individuals, as lesions in visible areas can lead to stigmatization. The duration of ulcers, with a high percentage presenting lesions for one month, emphasizes the need for early diagnosis and intervention. Early identification is essential due to the chronic nature of the disease, which can lead to significant morbidity and complications if left untreated [12].
In our study involving 94 patients with confirmed CL, we found that 50% of the lesions had a duration of one month, indicating a significant proportion of patients presented with relatively acute lesions. The breakdown of lesion duration among patients shows that while many patients seek treatment in the early stages of the disease, a significant number of individuals remain with longer-lasting lesions, which can potentially lead to complications. The duration of lesions is critically important in clinical manifestations of CL, as prolonged lesions can lead to more severe tissue damage and an increased risk of secondary infections [12]. Furthermore, early diagnosis and treatment are vital to preventing the progression of lesions and minimizing the associated morbidity [11]. Timely intervention can not only reduce the duration of lesions but also improve the overall quality of life for affected individuals [13].
The reliance on molecular methods such as PCR for diagnosis is a strength of this study. PCR not only aids in confirming the presence of L. major but also enhances species identification accuracy over traditional microscopy. As noted in the literature, these molecular techniques have transformed our understanding of leishmaniasis epidemiology by enabling strain characterization and monitoring genetic diversity within populations [26].
The absence of L. tropica in the sampled patients reflects findings from other studies in southwestern Iran, reinforcing the notion of regional variation in Leishmania species distribution [14, 21]. Given that L. tropica is associated with anthropogenic factors and urban environments, the results indicate a potential shift in environmental and ecological dynamics influencing Leishmania transmission in the region [13].
The increase in CL cases in Dezful may also be influenced by environmental changes and socio-economic factors, including urbanization, climatic fluctuations, and population migrations [13, 23]. As highlighted by Rejali et al. (2022), understanding how climate patterns correlate with CL outbreaks is crucial for predicting and mitigating future occurrences in endemic regions [26]. Furthermore, the socio-economic landscape in Dezful, which may involve insufficient public health infrastructure and a lack of community awareness about CL, necessitates targeted educational campaigns and health initiatives [2].
Given the predominance of L. major, ongoing surveillance and control measures are paramount in effectively managing CL in Dezful. Interventions should focus on vector control strategies, community education about transmission and prevention, and improving access to diagnostic and therapeutic resources [5, 27]. Collaborations between public health officials and local communities can enhance patient understanding of the disease and promote active participation in prevention efforts [28].
Clinical evidence in CL patients in this county has shown the presence of atypical lesions, including sporotrichoid, erysipelas-like, verrucous, and impetigo lesions. Additionally, instances of relapse, treatment failure, and drug resistance during the treatment of these patients underscore the necessity for more extensive studies, especially in the area of drug resistance genes.
While providing significant insights into the molecular identification of CL in Dezful City, this study also has limitations, such as the sample size. Although the number of 94 patients is sufficient for initial findings, it may limit the generalizability of the results. A larger sample size could provide a more comprehensive understanding of the epidemiological patterns of CL in the region. Since the study was conducted in a single city, the findings may not accurately represent other endemic areas of Khuzestan province or Iran. Therefore, multicenter approaches that encompass diverse geographical locations should be considered for future studies. To increase the effectiveness of public health responses to CL in Dezful, improvements in diagnostic methods, public education on CL transmission routes and prevention strategies, vector control, and strengthening of health care infrastructure are recommended. Future research should focus on several key areas to further understand and combat CL in Dezful City, including investigating the mechanisms of drug resistance in Leishmania species, especially L.major, determining the molecular characterization of Leishmania species, including investigating genetic diversity and pathogenicity, conducting longitudinal studies to monitor the incidence and prevalence of CL over time, and further research to understand the impact of environmental changes, climate fluctuations, and socioeconomic factors on the dynamics of CL transmission in Dezful and similar areas.
CONCLUSION
In conclusion, the findings of this study underscore the necessity of continued research and public health planning in tackling Cutaneous Leishmaniasis (CL) in Dezful City. The integration of molecular techniques and a comprehensive understanding of demographic and environmental factors will be instrumental in devising effective strategies to combat this re-emerging public health challenge.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATION
| CL | = Cutaneous Leishmaniasis |
| PCR | = Polymerase Chain Reaction |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was conducted following the ethical guidelines approved by the Ethics Committee of Dezful University of Medical Sciences, Khuzestan, Iran (IR.DUMS.REC.1401.060).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed oral consent was obtained from all participants, ensuring confidentiality and anonymity of patient information in line with ethical research practices.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
This article is an approved plan from the Deputy of Research, Dezful University of Medical Sciences, Khuzestan, Iran (MED-401043-1401).

