All published articles of this journal are available on ScienceDirect.

HCV Antibody Prevalence and Genotype Evolution in a Teaching Hospital, Calabria Region, Southern Italy Over A Decade (2008-2018)
Authors Info & Affiliations
Abstract
Background:
Hepatitis C Virus (HCV) infection is associated with a high risk of developing liver diseases. Globally, HCV prevalence is changing due to improving health care procedures, population movement, and availability of new antiviral therapy. In Italy, data on the prevalence of HCV infection are insufficient, out-dated, and restricted to specific areas.
Objective:
Between 2008 and 2018, we investigated HCV antibody (Ab) seroprevalence and genotypes distribution among patients presenting for testing at our Teaching Hospital.
Methods:
The HCV Ab and genotyping assays were performed by routine diagnostic methods. Chi-square for linear trend was carried out by OpenEpi (v3.01).
Results:
Among 120,009 consecutive patients, 5877 subjects were HCV Ab positive (4.89%). During the observational period 2008-2018, prevalence decreased significantly (p<0.001) from 4.7% in 2008 to 3.6% in 2018. HCV1b was the most prevalent subtype (47.2%) followed by HCV2a/2c (20.2%), and HCV3 (9.7%), while HCV4 showed a rate of 6.1%. HCV infection was more frequent in males (55.4%) than in females (44.6%). Overall, most infected patients were born before 1949.
Conclusion:
Epidemiological analyses are important to understand the evolution of the HCV epidemics under the influence of several factors, such as risk behaviour and therapy with direct-acting antivirals.
1. INTRODUCTION
Hepatitis C Virus (HCV) infection affects approximately 71 million people worldwide. It may cause chronic diseases and is responsible for liver-related complications (such as cirrhosis or hepatocellular carcinoma) [1]. Prevalence of HCV infection is different across different Countries: 3.5% in Asia and the Middle East, from 1.5% up to 3.5% in Southeast Asia, Latin America, Caribbean, Oceania and sub-Saharan, and lower than 1.5% in America and North America [2]. In Northern and Central Europe, HCV prevalence ranges from 0.2% to 1.2%, while in the Mediterranean area the overall prevalence ranges between 2.5% and 3.5%. In Italy, the Southern regions are endemic areas with a higher prevalence of HCV infection than the Northern ones [3]. Moreover, several factors may influence HCV incidence and prevalence over time. In fact, change of risk behaviour and more recently prescription of Direct-Acting Antivirals (DAAs) containing therapy may have produced positive effects on epidemics, which need to be explored.
HCV displays high genetic diversity; the distribution of genotypes and subtypes varies according to risk factors and geography. HCV1b is spread worldwide, HCV3a is prevalent in Europe and North America, HCV4 is endemic in the Middle East and Central Africa. HCV5 and HCV7 are responsible for less than 1% cases in the World, whereas HCV2 and HCV6 are responsible for around 23% cases. Recently, the new HCV8 was identified in patients from Punjab (India) [4, 5].
Epidemiology of HCV genotypes and subtypes is rapidly changing due to the movement of populations around the world and infection reservoirs in risk categories [6]. Ultimately, the introduction of DAA containing therapy may have modified the relative prevalence of HCV genotypes favouring the emergence of difficult-to-treat genotypes with respect to the more responding ones.
Over the last years, we performed an epidemiological analysis of genotype/subtype distribution in the Calabria Region [4, 6]. In the past, HCV1b was the most prevalent, followed by HCV2a/2c. HCV3 was the third most frequent and genotype HCV4 showed a higher prevalence compared to the National data. In particular, the presence of HCV4d was associated with Intravenous Drug Use (IDU) and blood transfusion as major risk factors, while HCV2c was mainly associated with the history of surgery, blood transfusions, and glass syringes use [6-9]. In the present study, we analysed the HCV types trend during eleven years (2008-2018) in our area. This period overlapped with previous analysis of genotypes prevalence, but data could not be combined due to different patient inclusion criteria [4, 6]. Additionally, in Italy, the HCV antibody (Ab) survey and types of epidemiological studies are out-dated and restricted to specific metropolitan areas or hospitals [10, 11]. More studies are needed to understand the real and updated infection prevalence and distribution of difficult-to-treat genotypes [12]. Therefore, for the first time, we assessed Ab prevalence and genotypes distribution of HCV in a sample of the general population coming to our hospital for HCV diagnostics procedures.
2. MATERIALS AND METHODS
We considered for our analysis all the sera of people who were screened for HCV infection and genotyping test in our centre between 1st January 2008 and 31st December 2018. Antibody data from the general population and genotype distribution from chronic patients were collected. HCV Ab screening was carried out by Elecsys® Anti-HCV II (Roche Diagnostics, Milan, Italy). Quantitative HCV RNA was performed by Cobas AmpliPrep/Cobas TaqMan HCV test (Roche Diagnostics, Milan, Italy). The 5’UTR and core amplified regions were analysed for genotyping by Versant HCV Genotype 2.0 Assay (Siemens, Healthcare Diagnostic Inc., Tarrytown, NY, USA), according to the manufacturer’s instructions. Detection of genotype 8 was not included in the routine assay. Ethical approval was not required due to the retrospective and noninterventional nature of the study. HCV Ab data were collected by FREQUENZA v12.5.3, available in METAFORA software. This tool does not allow to stratify patients by age, gender, and other characteristics. Chi-square (χ2) for a linear trend was performed by using OpenEpi (Version 3.01). Mean age (± standard deviation) of males and females were compared by Student test from quantitative data. A p-value < 0.05 was considered to be statistically significant.
3. RESULTS
3.1. HCV Antibody Prevalence Over Time
During the study period, 120,009 new consecutive patients were screened for HCV infection. Among these, 5877 (4.9%) subjects were found to be HCV Ab positive. The annual prevalence of HCV Ab significantly decreased from 4.7% in 2008 to 3.6% in 2018 (p<0.001). The highest annual prevalence was found in 2011 (5.5%). The trend of HCV Ab prevalence over time is shown in Fig. (1) (red line).
3.2. Genotype and Subtype Distribution
Genotyping was performed on 1,525 sera from as many viremic patients. Mean age (± standard deviation) was 58 (±15) years in males and 66 (±14) years in females. Females were significantly older than males (p<0.001). The complete pattern of HCV genotype/subtype prevalence over time is shown in Fig. (2). Overall, HCV1b and HCV2a/2c were the most prevalent subtypes (47.2% and 20.2%, respectively). HCV1b prevalence increased significantly (p<0.001) during the study period, with a peak in 2015 (57.2%); by contrast, the relative prevalence of HCV1a significantly decreased from 2008 (8.6%) to 2018 (1.1%) (p<0.001). The prevalence of HCV 2a/2c did not vary significantly over time with a peak in 2017 (25.4%). HCV3 showed a peak of 13.3% during 2014, and a nonsignificant trend from 2008 (10.9%) to 2018 (10.2%). HCV4 decreased from 4.7% in 2008 to 3.4% in 2018 reaching a peak in 2013 (9.3%). HCV3 was the third most frequent (9.7%) genotype. HCV4 showed a rate of 6.1%. Two HCV5 (< 1.0%) were found, while HCV6 and 7 were not detected. Mixed genotypes were found in ten (0.65%) cases.
In this patient sample, males were more frequent (55.4%) than females (44.6%). Particularly HCV3 was significantly more common in male patients compared to female ones (15.01% vs 2.8%; p<0.001). HCV1b and HCV2a/2c were significantly more frequent in females compared to males: 41.73% (353/846) vs. 54.05% (367/679) (p<0.001) and 17.49% (148/846) vs. 23.56% (160/679) (p=0.003), respectively. HCV1, HCV2, HCV1a and HCV4 genotype distribution did not display significant differences between genders (Table 1).
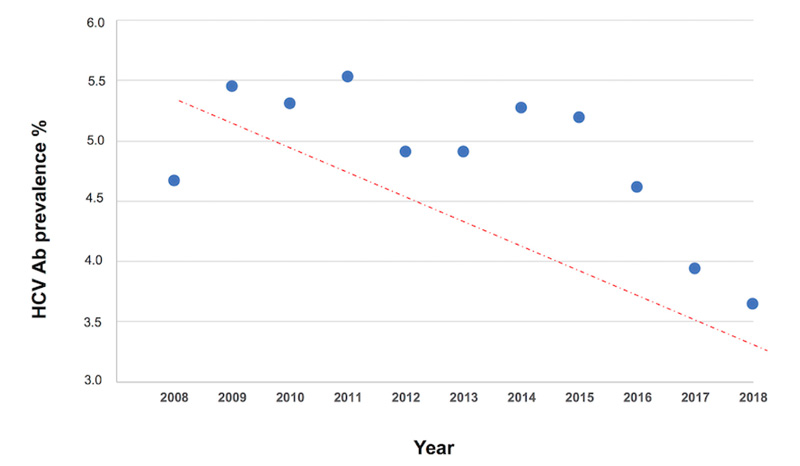
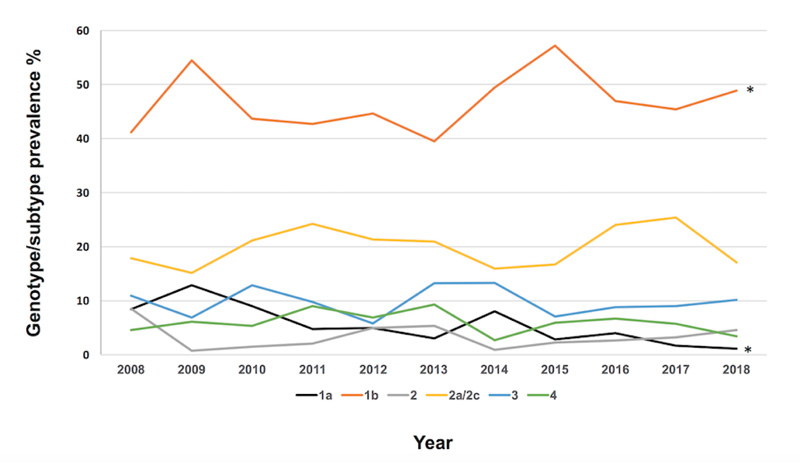
Table 1.
| Genotype/subtype | Male | Female | - | ||
| N | % | N | % | p value | |
| 1 | 68 | 8.04 | 39 | 5.74 | 0.08 |
| 1a | 52 | 6.15 | 29 | 4.27 | 0.1 |
| 1b | 353 | 41.73 | 367 | 54.05 | <0.001 |
| 1a/1b | 3 | 0.35 | 5 | 0.74 | 0.3 |
| 2 | 29 | 3.43 | 21 | 3.09 | 0.71 |
| 2a/2c | 148 | 17.49 | 160 | 23.56 | 0.003 |
| 3 | 127 | 15.01 | 19 | 2.80 | <0.001 |
| 4 | 58 | 6.86 | 35 | 5.15 | 0.16 |
| 5 | 1 | 0.12 | 1 | 0.15 | 0.87 |
| mixed | 7 | 0.83 | 3 | 0.44 | 0.35 |
| Total | 846 | - | 679 | - | - |
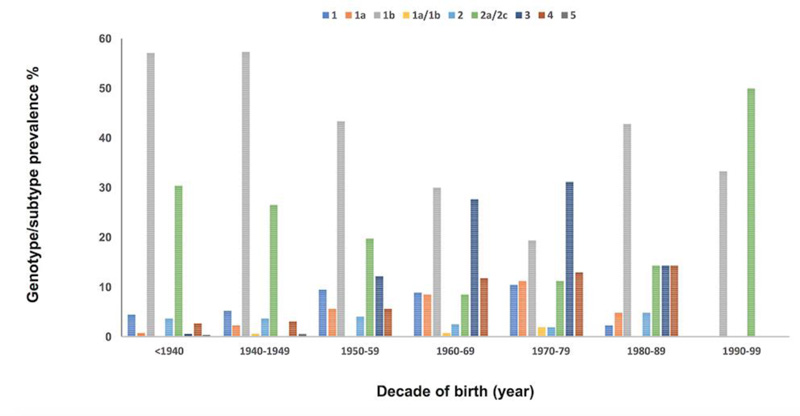
Most people who presented detectable HCV RNA with genotype testing were born before 1949. Particularly, in patients born from 1940 to 1949, the most frequent HCV genotype was 1b. By contrast, in patients born from 1990 to 1999, the most frequent genotype was HCV2a/2c, in those born from 1969 to 1977 HCV1a and HCV3 were most frequent, and in patients born between 1980 to 1989, HCV4 was most frequent (Fig. 3).
Coinfections with HIV or HBV were diagnosed in 21 and 7 patients, respectively, all born before 1968. HCV/HIV co-infected patients were mainly intravenous drug users and HCV3 was found to be the most prevalent genotype (10/21, 47.6%).
4. DISCUSSION
To date, this is the first and the biggest study which specifically evaluated both HCV Ab seroprevalence and genotype distribution in Southern Italy. The observed decrease of HCV Ab seroprevalence could be considered as a result of combined actions implemented to eradicate HCV infection (i.e., prevention of the infection due to stopping the use of glass syringes, screening campaigns or eradicating treatments through new drugs) [1]. In this regard, a limitation of this study is the lack of a stratified analysis of patients by age, gender and other relevant characteristics to understand in particular whether the significant decrease of HCV Ab over time may be due to a trend in specific subgroups. For instance, if in a given year more males were sampled and males have a higher prevalence of individuals who are positive for HCV Ab, then the higher observed HCV seroprevalence in that year may be explained by a higher percentage of males in the same year. Unfortunately, the software program used in our laboratory did not allow us to perform any stratification, so this kind of analysis needs to be done in further studies.
The success rate in HCV eradication is related to the availability of DAAs, even if several studies have reported possible collateral damages [13-16] and impaired achievement of sustained virological response due to genetic variants [17-19]. Nowadays, resistance-associated substitutions (RASs) are responsible for about 5% of virological failure cases. Therefore, even if the response rate with DAAs is extremely high, the potential risk of failure should be taken into account. Therefore, genotyping has to be performed at least in selected cases [12, 20-22]. HCV genotype distribution is continuously influenced by several factors such as the propensity of endemic genotypes to spread more around the world, changing transmission route (from the middle-aged “baby boomers” males to a new generation of young adults), according to specific areas [23-26]. Therefore, informative and preventative campaigns should be continued with a particular focus on emerging risk groups.
As for genotype distribution, the overall trend observed in this study showed a significantly decreased prevalence of HCV1a from 2008 (8.6%) to 2018 (1.1%), similar to data previously reported [27]. By contrast, HCV1a appeared to have similar distribution between genders, while it is significantly increased in males in West Europe, Russia and Israeli regions [27]. HCV1b (47.5%) is confirmed to be the predominant type and its prevalence increased significantly from 2008 (41.4%) to 2018 (48.9%) [28]. HCV1b was found mainly in females born between 1950-1959, while previously it was associated with elderly age [4, 6] or in those younger than 40 years of age [29]. HCV 2a/2c was the second most prevalent subtype (20.3%) in our Region. This subtype was significantly associated with female gender (23.5%). In Southern Italy, the relative prevalence of HCV2 increased from 2012 to 2014 (+7.0%), and it was high in people aged from 51 up to 60 years [29].
Overall, HCV3 prevalence (the third most frequent genotype in our population) increased in the Mediterranean area, except in Italy where a decreasing trend (-3%) was observed [28]. In the present analysis and in line with the previous studies, HCV3 was found mainly in males born between 1968 and 1977 [4, 6]. Recently, a moderate increase in HCV3a has been reported among young people in Southern Italy [29]. HCV4 genotype had a high prevalence until 2017 (6.7%), but it constantly decreased in the last decade. Our result is not consistent with published data which reported an increasing trend (+3%) in Italy, Greece, and Spain [28]. HCV4 is now related to young males. By contrast, HCV4 was mostly present in patients 56 - 65 years old (31.6%) in past observations [4, 6]. In conclusion, while we found the evolution of the relative prevalence of HCV genotypes, suggesting a nonresponse of some genotypes to specific drug combinations, our experience recently showed that all patients who were treated with DAA achieved SVR [30]. This may indicate that genotype evolution could be related, from the advent of pan-genotypic treatments, more to epidemiological pathways of transmission, which should be controlled.
However, as previously mentioned, genotyping is crucial to predict and tailor the most appropriate treatments in patients with possible RAS. Indeed, the European Association for the Study of the Liver (EASL) guidelines recommend to detect RAS before treatment, since the prevalence of RAS is heterogeneous (worldwide, among HCV genotypes and age stages) and may predict treatment response [31-35]. For this purpose, using Next-Generation Sequencing approach with analysis software packages could be really useful [19, 36]. Also, the study of resistances in association with phylogenetic analysis for each genotype/subtype may be useful to choose the eligible therapy [37].
CONCLUSION
In conclusion, epidemiological analyses are important to understand the evolution of the HCV epidemics under the influence of several factors such as risk behaviour and the effect of DAA containing therapy. The decrease of HCV Ab prevalence has evolved containment. What is the main driver of such evolution needs to be investigated in further studies. Moreover, it is important to monitor the relative prevalence of HCV genotypes so that the possible emerging routes of transmission can be understood and controlled.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
HCV Ab data were collected by FREQUENZA v12.5.3, available in METAFORA software.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

