All published articles of this journal are available on ScienceDirect.

Study of Hepatitis E Virus in Blood Donors
Abstract
Introduction:
Hepatitis E (HEV) is a major health problem affecting around one third of the world population. The prevalence of antibodies to HEV among blood donors have been documented in several countries in Europe and Asia.
Objectives:
The aims of the study are to estimate the seroprevalence of hepatitis E antibodies among healthy blood donors and to explore the factors associated with positive HEV antibodies among healthy blood donors. Moreover, to detect HEV viremia by real time polymerase chain reaction among seropositive blood donors for HEV.
Methods:
The study included 200 apparent healthy blood donors from Dakahlia Governorate, Egypt. Blood samples were collected from the blood donors for serological determination for specific hepatitis E virus immunoglobulin G (anti-HEV IgG) and specific hepatitis E virus immunoglobulin M (anti- HEV IgM). Positive samples for anti-HEV IgM were further subjected for determination of HEV-RNA by real time Polymerase Chain Reaction (PCR). Anti-HEV-IgG was positive in 50 donor (25%) anti-HEV-IgM was positive in 10 donors (5%) and HEV-RNA was positive in 6 donors (3%).
Results and Discussion:
The comparison between blood donors positive for anti-HEV-IgG and negative blood donors negative reveals significant association between anti-HEV-IgG and donors with older age (42.0 ± 9.7,P = 0.001),rural residence (76%, P = 0.001), workers in agricultural works (92%, P = 0.035) and elevated AST (31.28±14.28, P = 0.04). Regarding viral markers, there was significant prevalance between positive anti-HCV-IgG and positive anti-HEV-IgG (P = 0.003). Univariate analysis for risk factors associated with positive anti-HEV IgG reveals significant prevalence with older age (P = 0.001), rural residence (P < 0.001), positive anti-HCV- IgG (P = 0.004) and increase in AST (P = 0.045). However, on Multivariate analysis HEV infection was independently prevalent with older age (P < 0.001) and rural residence (P = 0.002).
Conclusion:
The present study highlights that HEV seroprevalence in blood donors is common finding. Further finding is the statistically significant correlation between antibodies to HCV and serological markers for HEV and even HEV viremia. Longitudinal studies may be needed to explore the clinical significance and cost effectiveness of screening of the blood donors for hepatitis E virus by serological tests and/or detection of viremia by Molecular testing.
1. INTRODUCTION
Hepatitis E Virus (HEV) is a nonenveloped, RNA virus, classified in the Genus Orthohepevirus of the Hepeviridae family. There are four different genotypes of HEV that are distributed in different geographical regions with different primary hosts [1]. Genotypes 1 and 2 affect humans only and genotypes 3 and 4 affect humans and animals and are transmitted zoonotically [2]. Genotype 1 is prevalent in Asia and Africa, whereas genotype 2 is prevalent in Central Africa and Central America [3]. Recently, a new genotype HEV 7 has been isolated from the Arabian Peninsula, mainly from the stool of the camels [4].
Hepatitis E (HEV) is a major health problem affecting around one-third of the population worldwide [5]. The prevalence of HEV is marked in the developing countries more than developed countries due to the reduced sanitary conditions affecting water supply and frequent contamination of the food leading to the outbreaks [5, 6]. Transfusion-transmitted hepatitis E virus (TT-HEV) has also been reported [7].
Infection with HEV leads to acute hepatitis either as sporadic cases around the year reported in all countries or as an outbreak in developing countries after flooding in the monsoon season [8].
The laboratory diagnosis of HEV infection depends on Serological tests and nucleic acid tests for detecting HEV-RNA.
The seroprevalence of anti-HEV IgG may reach up to 45% among healthy blood donors in the endemic countries [9]. In developed countries, the prevalence of antibodies to HEV among blood donors is contradictory and ranges from about 2% to 87% [10, 11].
This high seroprevalence grasps the attention of the possibility of the transmission of HEV in the blood transfusion. The risk of transmission from a donor with asymptomatic viremia can be identified through the detection of HEV RNA by Nucleic Acid Test (NAT) [7].
There are few reports from Egypt about the seroprevalence of antibodies to HEV.
The aims of the study were to estimate the seroprevalence of hepatitis E antibodies among healthy blood donors and to explore the factors associated with positive HEV antibodies among healthy blood donors. Moreover, to detect HEV viremia by real-time polymerase chain reaction among seropositive HEV-IgM blood donors.
2. MATERIALS AND METHODS
This cross-sectional study included 200 healthy blood donor volunteers attending blood banks in Mansoura University Hospital, Egypt from January 2017 till January 2018. The study was approved by the Mansoura Faculty of Medicine ethical committee and consent was obtained from each subject. The inclusion criteria were healthy blood donors above the age of 18 years. Rejected blood donors for medical illnesses were not included in the study. A complete medical history and clinical examination were performed for each subject.
Ten milliliter blood sample was obtained from each subject and sera were separated for liver function tests including albumin, total bilirubin, Aspartate Aminotransferase (AST) and Alanine Aminotransferase (ALT) by autoanalyzer (Dialab-GmbH, Germany) and complete serological markers for the detection of anti-hepatitis C virus IgG (anti-HCV IgG), Hepatitis B virus surface antigen (HBsAg) and hepatitis E virus.
2.1. Serologic Testing for HEV
Sera samples were tested for the presence of anti- HEV IgG and anti-HEV IgM by enzyme-linked immunosorbent assay (ELISA) by the use of the Wantai kit (Biological Pharmacy Enterprise Co., Ltd, Beijing, China) according to the instructions of the manufacturer. Antigens used in HEV IgM assay and HEV IgG assay are encoded by a structural region of open reading frame (ORF)-2 from an isolate of genotype HEV genotype 1 [2].
Serum samples that gave an absorbance value greater than the cut off value were considered to be positive for HEV antibodies.
Positive samples for anti-HEV IgM were further subjected to detect HEV-RNA by real-time polymerase chain reaction.
2.2. Detection of HEV RNA
2.2.1. Extraction of RNA
RNA of HEV was extracted from 200 µL of the serum sample by the use of viral RNA extraction kit from body fluids (QIAamp viral RNA mini kit, Qiagen) according to the instructions of the manufacturer. The extracted RNA was kept at -80°C for further reverse transcription real-time Polymerase Chain Reaction (PCR).
2.2.2. Reverse-Transcriptase Real-Time PCR (RT-PCR)
RT-PCR was used to detect HEV genes, as previously described [12]. RT-PCR was performed by the use of 10 µL of the extracted RNA according to the instructions of the manufacturer of a qualitative HEV RT-PCR kit (RealStar® HEV RT-PCR Kit) using an RT-PCR instrument (QIAGEN's real-time PCR system, Rotor-Gene Q).
Briefly, the test involves a real-time RT-PCR system. It uses specific primers and a double-marked probe for the amplification and detection of Hepatitis E Viral (HEV) RNA. The test primarily consists of two stages: (1) Extraction of RNA from patient samples, (2) Reverse Transcription (RT), amplification and detection of a specific target molecule. To ensure that the nucleic acids isolated from the patient samples do not contain any PCR-inhibiting substances, the sample is subjected to Internal Control (ICR) prior to isolation. This ICR is transcribed to cDNA, amplified and detected in the same RT-PCR preparation. In this way, false-negative results due to inhibition of the RT-PCR reaction can be excluded. Probes for the specific detection of HEV RNA are marked with the reporter dye FAM. Probes for the detection of Internal Control (ICR) are marked with yellow dye. It is thus possible to detect both target sequences in a single reaction. Cycle Thresholds (CT) were calculated according to the instructions of the manufacturer, HEV RNA viral load was calculated in copies per reaction. Positive samples for HEV-RNA were studied for the genotype of HEV according to qualitative RT-PCR assays for ORF 1, ORF 2, and ORF2/3 with subsequent sequencer study [12].
2.3. Statistical Methods
Data were analyzed using Statistical Package for Social Science software computer program version 22 (SPSS, Inc., Chicago, IL, USA). Quantitative parametric data were presented in mean and standard deviation, while qualitative data were presented as frequency. Student’s t-test (unpaired) was used for comparing quantitative parametric data, while chi-square “χ2”, Fischer’s exact tests or Monte-carlo, as indicated, were used to compare the qualitative data. Univariate & multivariate logistic regression for anti- HEV IgG was done to detect predictive factors. P-value less than 0.05 was considered statistically significant.
3. RESULTS
This study included 200 apparent healthy blood donors with a mean age of 36.1 ± 9.6 with the predominance of the male gender (69%). The residence of the donors was equal in distribution. For the virologic markers of hepatitis viruses, anti-HCV-IgG was positive in 12%, HBsAg was positive in 2%, anti-HEV -IgG was positive in 25%, anti-HEV-IgM was positive in 5%, and HEV-RNA was positive in 3%, (Table 1).
The comparison between blood donors positive for anti-HEV-IgG and negative blood donors reveals statistically significant prevalence between anti- HEV-IgG and donors with older age (42.0 ± 9.7, P = 0.001), rural residents (76%, P = 0.001), workers in agricultural areas (92%, P = 0.035) and elevated AST (30.28 14.28, P = 0.04). Regarding viral markers, there was a statistically significant correlation between positive anti-HCV- IgG and positive anti- HEV- IgG (24%, P = 0.003)), (Table 2).
The comparison between blood donors positive for anti-HEV-IgM and negative blood donors reveals significant prevalence between anti HCV- IgG (40%, P = 0.02), HBsAg (20%, P = 0.001), and HEV-RNA (60%, P = 0.001). Both AST and ALT had significant elevated levels in blood donors positive for HEV-IgM (P = 0.01, P = 0.001, respectively). Moreover, blood donors positive for HEV-RNA, revealed a statistically significant prevalence between anti-HCV-IgG (66.7%, P = 0.002), HBsAg (33.3%, P = 0.004) and elevated ALT (48.3 2.6, P = 0.002), (Tables 3 and 4). The genotype of HEV-RNA samples revealed genotype 1 for all samples, data not shown.
Univariate analysis for risk factors associated with positive anti-HEV IgG reveals high prevalence with older age (OR 1.095-CI: 1.055-1.137, P = 0.001)), rural residents (OR 0.22-CI: 95: 0.108-0.46, P<0.001), positive anti-HCV-IgG (OR 3.63 CI 95%: 1.51-8.7, P = 0.004), and increase in AST (OR 1.02, CI95% 1.00-1.05, P = 0.045). However, in multivariate analysis HEV infection was independently associated, only with older age OR 1.080, CI95% 1.034-1.1281.034 P < 0.001 and rural residents (OR 0.279, CI95% 0.125-0.620 P = 0.002), (Table 5).
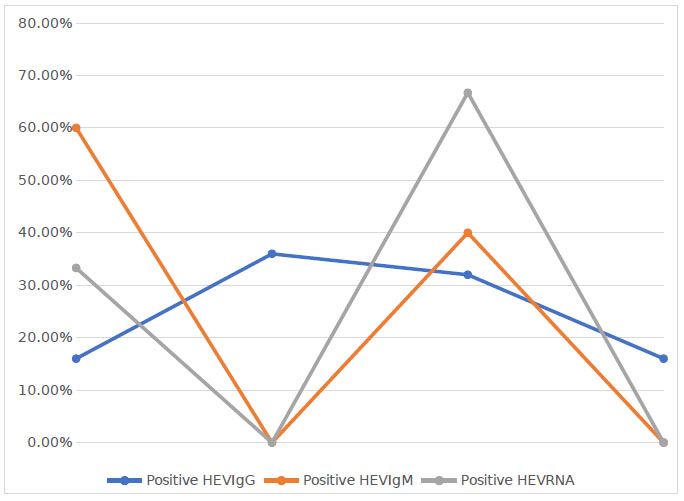
Age analysis for positive HEV-IgG reveals a significant increase in positive HEV-IgG in the age group of 35-44 years with a significant increase in HEV-IgM in younger age group (18-34 years, P = 0.01), and HEV-RNA showed a significant increase in age group (45-55), (Fig. 1).
| Age | 36.05±9.64 | ||
|---|---|---|---|
| Albumin(g/dl) | 4.27±.39 | ||
| Total bilirubin (mg/dl) | .71±.34 | ||
| AST (IU/L) | 28.20±12.44 | ||
| ALT(IU/L) | 31.84±13.27 | ||
| Sex | Male | 138 | 69.0% |
| Female | 62 | 31.0% | |
| Residence | Rural | 100 | 50.0% |
| Urban | 100 | 50.0% | |
| Anti- HCVIgG | Negative | 176 | 88.0% |
| Positive | 24 | 12.0% | |
| HBs Ag | Negative | 196 | 98.0% |
| Positive | 4 | 2.0% | |
| Anti-HEV IgG | Negative | 150 | 75.0% |
| Positive | 50 | 25.0% | |
| Anti-HEV IgM | Negative | 190 | 95.0% |
| Positive | 10 | 5.0% | |
| HEV-RNA | Negative | 194 | 97.0% |
| Positive | 6 | 3.0% | |
| – | HEV-IgG | |||||
|---|---|---|---|---|---|---|
| Negative | Positive | P | ||||
| Age | 34.07±8.79 | 42.00±9.70 | <0.001* | |||
| Albumin (g/dl) | 4.28±.41 | 4.23±.35 | 0.48 | |||
| Total bilirubin (mg/dl) | 70±.35 | .73±.31 | 0.5 | |||
| AST(IU/L) | 27.17±11.64 | 31.28±14.28* | 0.04* | |||
| ALT(IU/L) | 31.03±13.95 | 34.28±10.74 | 0.13 | |||
| Sex | Male | 106 | 70.7% | 32 | 64.0% | 0.37 |
| Female | 44 | 29.3% | 18 | 36.0% | ||
| Residence | Rural | 62 | 41.3% | 38 | 76.0% | <0.001* |
| Urban | 88 | 58.7% | 12 | 24.0% | ||
| Anti- HCV-IgG | Negative | 138 | 92.0% | 38 | 76.0% | 0.003* |
| Positive | 12 | 8.0% | 12 | 24.0% | ||
| HBs-Ag | Negative | 148 | 98.7% | 48 | 96.0% | 0.26 |
| Positive | 2 | 1.3% | 2 | 4.0% | ||
| Education | Educated | 144 | 96.0% | 46 | 92.0% | 0.27 |
| Non-educated | 6 | 4.0% | 4 | 8.0% | ||
| Work | Agricultural workers | 148 | 98.7% | 46 | 92.0% | 0.035* |
| Non-Agricultural workers | 2 | 1.3% | 4 | 8% | ||
* significance <0.05 Test used: Student’s t-test for data expressed as mean±SD and Chi-square or Fisher’s exact test for data expressed as frequency
| – | HEV-IgM | |||||
|---|---|---|---|---|---|---|
|
Negative (n=190) |
Positive (n=10) |
P | ||||
| Age | 36.19±9.39 | 33.40±13.88 | 0.37 | |||
| Albumin (g/l) | 4.27±.40 | 4.16±.28 | 0.38 | |||
| Total bilirubin (mg/dl) | 0.70±.34 | 0.74±.25 | - | |||
| AST(IU/L) | 27.68±12.35 | 38.00±10.33 | 0.01* | |||
| ALT(IU/L) | 31.15±13.20 | 45.00±5.77 | 0.001* | |||
| Sex | Male | 132 | 69.5% | 6 | 60.0% | 0.5 |
| Female | 58 | 30.5% | 4 | 40.0% | ||
| Residence | Rural | 96 | 50.5% | 4 | 40.0% | 0.7 |
| Urban | 94 | 49.5% | 6 | 60.0% | ||
|
Anti- HCV-
IgG |
Negative | 170 | 89.5% | 6 | 60.0% | 0.02* |
| Positive | 20 | 10.5% | 4 | 40.0% | ||
| HBs-Ag | Negative | 188 | 98.9% | 8 | 80.0% | 0.01* |
| Positive | 2 | 1.1% | 2 | 20.0% | ||
P: Probability *significance <0.05.
Tests used: Student’s t-test for data expressed as mean ± SD and Chi-square or Fisher’s exact test for data expressed as frequency.
| – | HEV-RNA | |||||
|---|---|---|---|---|---|---|
|
Negative (n=194) |
Positive (n=6) | P | ||||
| Age | 35.92±9.48 | 40.33±14.21 | 0.27 | |||
| Albumin(gm/L) | 4.27±.40 | 4.10±.18 | 0.29 | |||
| Total bilirubin (mg/dl) | 0.70±.34 | 0.80±.31 | 0.49 | |||
| AST(IU/L) | 27.94±12.35 | 36.67±13.66 | 0.09 | |||
| ALT(IU/L) | 31.33±13.14 | 48.33±2.58 | 0.002* | |||
| Sex | Male | 134 | 69.1% | 4 | 66.7% | 1.00 |
| Female | 60 | 30.9% | 2 | 33.3% | ||
| Residence | Rural | 96 | 49.5% | 4 | 66.7% | 0.68 |
| Urban | 98 | 50.5% | 2 | 33.3% | ||
|
Anti- HCV- IgG |
Negative | 174 | 89.7% | 2 | 33.3% | 0.002* |
| Positive | 20 | 10.3% | 4 | 66.7% | ||
| HBs-Ag | Negative | 192 | 99.0% | 4 | 66.7% | 0.004* |
| Positive | 2 | 1.0% | 2 | 33.3% | ||
| – | Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|---|
| P | OR | 95%CI | P | OR | 95%CI | ||
| Age | <0.001* | 1.095 | 1.055-1.137 | <0.001* | 1.080 | 1.034-1.128 | |
| Sex | Female/ Male | .378 | 1.355 | .689-2.664 | – | – | – |
| Residence | Urban /Rural | <0.001* | .222 | .108-.460 | .002* | .279 | .125-.620 |
| Albumin (g/dl) | .480 | .742 | .324-1.698 | – | – | – | |
| Total bilirubin (mg/dl) | .520 | 1.332 | .556-3.189 | – | – | – | |
| AST(IU/L) | .045* | 1.026 | 1.001-1.051 | .087 | 1.026 | .996-1.056 | |
| ALT(IU/L) | .136 | 1.018 | .994-1.042 | – | – | – | |
| Anti- HCV-IgG | Positive /Negative | .004* | 3.632 | 1.511-8.729 | .949 | 1.037 | .342-3.139 |
| HBs-Ag | Positive /Negative | .267 | 3.083 | .423-22.485 | – | – | – |
| HEV-IgM | Positive /Negative | .270 | 2.087 | .564-7.719 | – | – | – |
| HEV-RNA | Positive /Negative | .035* | 6.435 | 1.142-36.272 | .128 | 4.363 | .655-29.052 |
4. DISCUSSION
Hepatitis E virus has emerged as a health problem in industrialized countries. In Egypt, it has been estimated that anti-HEV-IgG is prevalent among 84% of the adults in rural regions and is considered as a zoonotic and anthroponotic viral infection [14]. There are various reports from different geographic locations that have determined an increase in the prevalence of HEV either due to real increase in the infections or due to the increase of the awareness of this infection [15].
There are some concerns about the used ELISA assays worldwide and among different laboratory kits for screening; however, the used kit in the present study, Wantai, is accepted as a sensitive and specific method [16, 17].
In the present study, anti-HEV IgG was positive in 25% of apparently healthy blood donors. There were variations in the seroprevalence of HEV that ranges from 20% to 86.4% [10, 13, 18]. In a previous study from Egypt among blood donors, the prevalence was 20.9% [19]. The prevalence depends upon many factors such as the age of the studied group, geographic location, work, education levels and gender distribution, variable levels of exposure to the virus, and the use of different serological testing kits.
In our study, the seroprevalence of anti-HEV-IgG was found higher with older age, rural residence and agricultural related work. Similar findings were reported in previous studies [20-22]. The association between older age and positive anti-HEV-IgG may reflect the cumulative lifetime contact frequency to HEV.
The association of agricultural work with anti-HEV-IgG reflects the zoonotic nature of HEV as those populations have frequent contact with animals [20], and also from lack of healthy water supply and environmental hygiene.
However, some studies reported no significant difference between people who lived in urban and rural areas in terms of hepatitis E prevalence [15].
The remarkable finding in the present study was the significant presence of anti-HEV-IgG with positive anti-HCV. Though a previous study did not find such an association among blood donors [23], other studies had found a strong association between anti-HEV-IgG and HCV antibodies in patients with chronic HCV infection [24-26]. This finding may reflect a common mode of transmission of these viruses. Blood products were found to be associated with HEV transmission in different studies [27, 28].
Both ALT and AST had significant elevated levels in blood donors positive for HEV-IgM (P = 0.01, P = 0.001).
Previous reports had similar findings [29-31]. Though the degree and duration of HEV viremia have not been directly correlated with ALT or HEV antibody levels [32], elevated ALT may be associated with asymptomatic HEV infections [33]. Thus, a question arises; whether screening of the blood donors by ALT and AST may be used as a clue for underlying HEV infection or not.
The transmission of HEV depends upon the presence of acute infection, especially viremia. HEV-IgM was positive in 10 (5%) donors, and HEV- RNA was detected in 6 (3%) cases of the blood donors. The incidence of HEV viremia in European studies ranges from 1:600 to 1:15000 [28, 34, 35], and several studies have documented HEV blood transfusion transmission [34, 36, 37]. The genotype of HEV was genotype 1. This finding was similar to the previous study from Egypt [12].
The higher prevalence of HEV viremia in the present study may be attributed to the nature of the population studied as they were mainly working in agricultural related work as Dakahlia Governorate is a rural region. The transmission of HEV in immunocompetent patients is usually self-limited and asymptomatic. However, in immunocompromised patients, such as patients with transplantation this virus may lead to chronic infections. Therefore, some European countries introduced the molecular screening of blood donation for HEV virus [27, 38].
However, the clinical significance of this screening in Egypt is actually unknown due to lack of reports about the HEV infection after blood transfusion due to the lack of specific symptoms and even the development of symptoms a long time after transfusion that hampers the association with previous blood transfusion practice [39].
CONCLUSION
The present study highlights that HEV seroprevalence in blood donors is a common finding. Further findings describe the presence of antibodies to HCV and serological markers for HEV and even HEV viremia. Longitudinal studies may be needed to explore the clinical significance and cost-effectiveness of screening of the blood donors for hepatitis E virus by serological tests and/or detection of viremia by molecular testing.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The ethical approval was obtained from the Institutional Review Board (IRB) of the Faculty of Medicine, Mansoura University, Egypt (code no. R/18.6.222).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent was obtained from all the participants.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article are available in the Figshare repository. The reference number is https://figshare.com/articles/Article/10311212.
FUNDING
None.
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

