All published articles of this journal are available on ScienceDirect.

Comparison of Effectiveness of Germania Honey Compared to Manuka Honey in Methicillin-Resistant Staphylococcus aureus (MRSA) Killing
Abstract
Purpose:
Manuka honey is currently used in medical-grade sterile wound treatment products and has been shown to be effective in methicillin-resistant Staphylococcus aureus (MRSA) killing in vitro and in wound healing in a number of case studies and series. Locally produced honey in Pakistan and Chile have been proposed to be as effective as Manuka honey in bacterial killing in vitro, presenting potentially more accessible and affordable alternatives. In this study, we compared the effectiveness of a local Germania honey from Saudi Arabia to Manuka honey MGO 550 for in vitro killing of MRSA.
Methodology:
Overnight Muller Hinton broth cultures of 50 wound culture isolates of MRSA from 50 patients were incubated with a series of dilutions of Manuka honey MGO 550 and corresponding Germania honey dilutions for 24 h. Turbidity was assessed to determine whether bacterial growth had occurred, and no growth was confirmed by a further 24 h sub-culture on blood agar.
Results/Key findings:
Manuka honey MGO 550 was significantly more effective than Germania honey at MRSA killing at 100% v/v, 50% v/v and 25% v/v (p=0.025, 0.000265, and 0.000112 respectively)
Conclusion:
Manuka honey MGO 550 is significantly more effective in killing MRSA in vitro than Germania honey. Germania honey does not appear to be a promising locally produced alternative to Manuka honey for the development of honey-based wound dressings. Further experiments could determine if Germania honey is effective against other bacterial species.
1. INTRODUCTION
The rise in antimicrobial resistance in bacteria is a major worldwide public health issue. In the context of bacterial Skin and Skin Structure Infections (SSSI), Skin and Soft Tissue Infections (SSTI) and wound infections, methicillin-resistance Staphylococcus aureus (MRSA) is of particular concern; the emergence of Vancomycin-Intermediate S aureus (VISA), heterogeneous VISA, and vancomycin-resistant S. aureus (VRSA) strains has further reduced antibiotic options [1-4]. Prevalence of MRSA among SSSIs and SSTIs varies geographically but is generally high. For example, in a study on 471,550 SSTI episodes in Northern California between 2009 and 2011, S. aureus was the pathogen identified in 81% of pathogen-positive specimens, of which 46% were MRSA, while in a retrospective review of 200 S. aureus isolates, of which 87.3% were SSTIs, in the western region of Saudi Arabia between 2009 and 2010, MRSA was found in 39.5% of isolates [1, 5]. Other important antibiotic-resistant bacteria in SSTIs are Enterobacteriaceae including Escherichia, Klebsiella, Citrobacter, Enterobacter and Serratia, such as Carbapenem-Resistant Enterobacteriaceae (CRE) and extended spectrum β-lactamase (ESBL)-expressing Enterobacteriaceae [6-8]. Pseudomonas aeruginosa persistence in chronic wounds due to the formation of biofilms and tolerance of many antimicrobial treatments is another serious public health issue [9]. The increasing prevalence of such infections has necessitated attempts to identify alternative antibiotic treatments and has also raised interest in non-antibiotic therapies.
Honey is an example of a remedy that has been used historically and in complementary medicine in wound dressings and is currently in use in sterile wound treatment products licenced in many countries [10, 11]. Most interest centres on Manuka honey, which is made from Leptospermum scoparium (Manuka) trees found in New Zealand and Australia [11, 12]. Antibacterial activity of many kinds of honey is related to levels of hydrogen peroxide; however, Leptospermum honey are relatively low in hydrogen peroxide and their antimicrobial activity correlates with levels of methyl glyoxal (MGO) which is produced by dehydration of dihydroxyacetone (DHA) from the nectar of the Manuka flowers [11-14]. While hydrogen peroxide or MGO are important elements of honey’s antibacterial activity, other mediators may also play a part, including defensins, glycosides and phenolic antioxidant compounds [11].
Sterile Manuka honey-based products such as Medihoney™ have been associated with infection clearance and wound healing in a number of case studies and series, for example in treatment of leg ulcers, as well as chronic Pressure Ulcers (PUs) in Spinal Cord-Injured (SCI) patients, wound care in pediatric oncology patients and prevention of pin site infections during open reduction with external fixation (OREF) for correction of Charcot deformity in diabetic patients [15-18]. Medical grade Manuka honey preparations have been shown to be effective in vitro against both biofilm and free-swimming bacteria, including MRSA and Pseudomonas aeruginosa [9, 19]. Synergism in vitro with rifampicin has also been observed against MRSA biofilms and free-swimming bacteria [20, 21]. The beneficial effects of Manuka honey in treating infection are mediated by various proposed mechanisms, including changes in gene and protein expression levels of mediators of bacterial ribosomal function, protein synthesis, stress responses, growth and metabolism [10, 22], down-regulation of expression of genes associated with virulence, cell division and the tricarboxylic acid cycle [23, 24] and reduction in expression of universal stress protein A [25].
Some studies have suggested that other locally produced kinds of honey from various regions including Pakistan and Chile are also effective antibacterial agents in in vitro studies [26, 27]. In this study, we compared the efficacy of local Germania honey from Saudi Arabia versus Manuka honey MGO 550 in the inhibition of growth of 50 MRSA patient samples.
2. MATERIALS AND METHODS
2.1. Bacterial Strains
50 wound culture isolates of MRSA from 50 patients were tested for sensitivity to either Manuka honey MGO 550 or a local Germania commercial honey product from Saudi Arabia. Clinical isolates were identified as MRSA using routine screening by Polymerase Chain Reaction (PCR) with the Xpert MRSA-SA Nasal Complete G3 kit. Overnight cultures of each strain were prepared in Muller Hinton broth. Antibiotic susceptibility profiles were determined according to the CLSI M100 2018 criteria [28]. Samples were primarily tested using an automated microbiology identification system (VITEK® 2; bioMerieux, Marcy-l’Etoile, France) system for sensitivity to the following antibiotics: penicillin, oxacillin, gentamicin, ciprofloxacin, levofloxacin, moxifloxacin, clindamycin, erythromycin, quinupristin, linezolid, vancomycin, tetracycline, tigecycline, nitrofurantoin, rifampicin and trimethoprim/ sulfamethoxazole and for Inducible Clindamycin Resistance (ICR). VITEK-2 tests for sensitivity were performed by calculating the Minimum Inhibitory Concentration (MIC) for each antibiotic, and the interpretation of each MIC value was assessed based on the CLSI guidelines [28]. ATCC33591 strain was used as the control. Cefoxitin was also used to determine the presence or absence of MRSA.
2.2. Honey Samples
Manuka Honey stock solution was made by mixing 108 g of Manuka honey MGO 550 (1 g contains 550 μg MGO) with 100 ml Muller Hinton broth to give a final MGO concentration of 600 μg/ml. 100 mg catalase was added to the stock solution to neutralize hydrogen peroxide. A series of two-fold dilutions of the stock solution were carried out in honey-free Muller Hinton broth to give final concentrations of 600 μg/ml (undiluted), 300 μg/ml (50% v/v), 150 μg/ml (25% v/v), 75 μg/ml (12.5% v/v) and 37.5 μg/ml (6.25% v/v) (1 ml per tube). A 0.5 McFarland suspension from each of the 50 overnight MRSA cultures was prepared and diluted to a cell density of 5 x 107 CFU/mL in 0.45 saline, and 5 x 105 CFU (10 μl) of each diluted bacterial suspension was transferred to each of the Manuka honey MGO 550-containing tubes to give a final bacterial concentration 5 x 105 CFU/ml, as per CLSI guideline recommendations. A commercial local Germania honey stock solution was prepared, diluted, and inoculated in the same way as for Manuka honey for comparison purposes. Bacterial growth was assessed by checking for turbidity in Muller Hinton broth after 24 h of culture. We used DensiCHEK™ Plus (bioMérieux) with the VITEK® 2 system to adjust the turbidity to zero after the samples were inoculated. 24 hours later, all samples that showed no growth by naked eye were confirmed using the DensiCHEK™ Plus device. For all tubes that were scored as clear, samples were sub-cultured on to blood agar plates which were incubated for a further 24 h to finally confirm no bacterial growth.
2.3. Data Analysis
To compare the distribution of growth versus non-growth results between Manuka honey MGO 550 and Germania honey at corresponding dilutions, Chi-squared analysis was used, with p≤0.05 accepted as significant. Statistical analysis was performed using Social Sciences Statistics and GraphPad QuickCalcs online software.
3. RESULTS
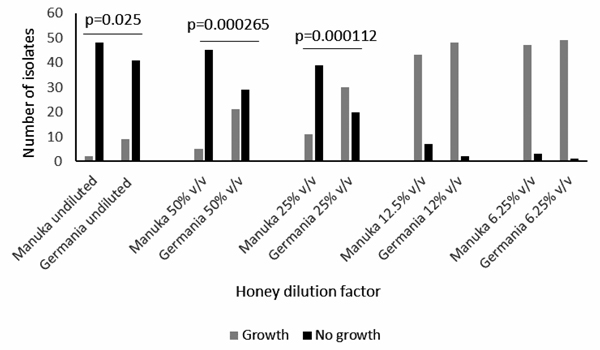
The number of isolates for which growth or no growth occurred was scored for each dilution of Manuka honey MGO 550 and Germania honey (Table 1), (Fig. 1). Undiluted Manuka honey (600 μg/ml) was significantly more effective than undiluted locally sourced Germania honey against MRSA (p=0.025) Table 1; Fig. (1). At 50% v/v and 25% v/v dilutions, Manuka honey was also significantly more effective in bacterial killing (p= 0.000265 and 0.000112 respectively) Table 1; Fig. (1). At 12.5% v/v and 6.25% v/v, both honey types were equally ineffective (Fig. 1); (Table 1), thus Manuka honey MGO 550 at concentrations of 75 μg/ml MGO was ineffective in MRSA killing in vitro.
Antibiotic resistance profiles for the 50 MRSA isolates are shown in Table 2. All strains were resistant to cefoxitin. 26 isolates had the same profile as the control ATCC33591 strain; the remaining 24 isolates were divided between seven further profiles. The number of isolates which grew in the presence of undiluted, 50% v/v, 25% v/v and 12.5% v/v dilutions for both Manuka and Germania honey was considered with respect to antibiotic resistance profile (Table 3). Consistent with the overall results, the growth of the dominant MRSA strain was significantly less on undiluted, 50% v/v and 25% v/v Manuka honey compared to Germania honey (Table 2). The small total number of isolates for each of the other antibiotic susceptibility profiles complicated analysis of any differences in effect between the two honey types (Tables 2 and 3).
| - | Bacterial Growth | - | - | ||
|---|---|---|---|---|---|
| - | Yes | No | ATCC 33591 | Chi square statistic | -P value |
| Manuka 600 μg/ml (undiluted) | 2 | 48 | No growth | 5.005 | 0.025 |
| Germania undiluted stock | 9 | 41 | No growth | ||
| Manuka 300 μg/ml (50% v/v) | 5 | 45 | No growth | 13.306 | 0.000265 |
| Germania (1/2 diluted) (50% v/v) | 21 | 29 | Growth | ||
| Manuka 150 μg/ml (25% v/v) | 11 | 39 | No growth | 14.923 | 0.000112 |
| Germania 1/4 diluted (25% v/v) |
30 | 20 | Growth | ||
| Manuka 75 μg/ml (12.5% v/v) | 43 | 7 | Growth | 3.052 | 0.081 |
| Germania 1/8 diluted (12.5% v/v) |
48 | 2 | Growth | ||
| Manuka 37.5 μg/ml (6.25% v/v) | 47 | 3 | Growth | 1.042 | 0.307 |
| Germania 1/16 diluted (6.25% v/v) | 49 | 1 | Growth | ||
| - | Number of strains | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 26 | 4 | 5 | 3 | 5 | 1 | 4 | 2 | 50 | |
| Antibiotic | |||||||||
| Penicillin | R | R | R | R | R | R | R | R | - |
| Oxacillin | R | R | R | R | R | R | R | R | - |
| Gentamicin | S | S | S | S | S | S | R | R | - |
| Ciprofloxacin | S | S | S | S | R | S | R | R | - |
| Levofloxacin | S | S | S | S | R | S | R | R | - |
| Moxifloxacin | S | S | S | S | S | S | S | R | - |
| Clindamycin | S | R | S | R | S | S | S | R | - |
| Erythromycin | S | R | S | R | S | S | S | R | - |
| Quinupristin | S | S | S | S | S | S | S | S | - |
| Linezolid | S | S | S | S | S | S | S | S | - |
| Vancomycin | S | S | S | S | S | S | S | S | - |
| Tetracycline | S | S | R | R | R | S | S | S | - |
| Tigecycline | S | S | S | S | S | S | S | S | - |
| Nitrofurantoin | S | S | S | S | S | S | S | S | - |
| Rifampicin | S | S | S | S | S | S | S | S | - |
| Trimethoprim/ sulfamethoxazole | S | S | S | S | S | R | S | S | - |
| ICR | NEG | POS | NEG | NEG | NEG | NEG | NEG | POS | - |
| ATCC33591 control strain profile | |||||||||
| - | Number of isolates with growth | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Man undiluted Ger undiluted |
2 7 |
0 2 |
0 0 |
0 0 |
0 0 |
0 0 |
0 0 |
0 0 |
2 9 |
| Man 50% v/v Ger 50% v/v |
4 18 |
1 2 |
0 1 |
0 0 |
0 0 |
0 0 |
0 0 |
0 0 |
5 21 |
| Man 50% v/v Ger 50% v/v |
8 25 |
2 2 |
0 1 |
0 0 |
1 2 |
0 0 |
0 0 |
0 0 |
11 30 |
| Man 50% v/v Ger 50% v/v |
25 26 |
4 4 |
2 5 |
2 2 |
3 4 |
1 1 |
4 4 |
2 2 |
43 48 |
| Antibiotic | |||||||||
| Penicillin | R | R | R | R | R | R | R | R | - |
| Oxacillin | R | R | R | R | R | R | R | R | - |
| Gentamicin | S | S | S | S | S | S | R | R | - |
| Ciprofloxacin | S | S | S | S | R | S | R | R | - |
| Levofloxacin, | S | S | S | S | R | S | R | R | - |
| Moxifloxacin | S | S | S | S | S | S | S | R | - |
| Clindamycin | S | R | S | R | S | S | S | R | - |
| Erythromycin | S | R | S | R | S | S | S | R | - |
| Quinupristin | S | S | S | S | S | S | S | S | - |
| Linezolid | S | S | S | S | S | S | S | S | - |
| Vancomycin | S | S | S | S | S | S | S | S | - |
| Tetracycline | S | S | R | R | R | S | S | S | - |
| Tigecycline | S | S | S | S | S | S | S | S | - |
| Nitrofurantoin | S | S | S | S | S | S | S | S | - |
| Rifampicin | S | S | S | S | S | S | S | S | - |
| Trimethoprim/ sulfamethoxazole | S | S | S | S | S | R | S | S | - |
| ICR | NEG | POS | NEG | NEG | NEG | NEG | NEG | POS | - |
4. DISCUSSION
In this study, we compared the in vitro performance of a locally sourced Germania honey against Manuka honey MGO 550 in killing MRSA from patient wound infections. Consistent with previous findings, Manuka honey was effective in preventing the growth of MRSA down to a dilution of 25% v/v [9, 19, 27]. However, unlike some other kinds of honey, including black seed honey from Pakistan or Ulmo 90 honey from Chile, diluted Germania honey was relatively ineffective against MRSA and it was significantly less effective than Manuka honey even when undiluted [26, 27]. One recent study comparing locally produced black seed honeys from Pakistan to Manuka honey showed that while Manuka honey was more effective, with a lower Minimum Inhibitory Concentration (MIC), than the other honeys against 25 wound cultures of MRSA and standard strains of S. aureus, P. aeruginosa and E. coli, the differences were minimal [26]. Importantly, the locally produced honeys may represent a more accessible and affordable solution [26]. Results of another study on Chilean honey made from the Ulmo tree (Ulmo 90 honey) showed that in agar diffusion and MIC spectrophotometric studies the Ulmo 90 honey was more effective than UMF® 25+ honey against five MRSA isolates and equivalent for P. aeruginosa and E. coli strains [27]. By contrast, our locally produced Germania honey does not appear to be a good potential local alternative to use of Manuka honey in the treatment of MRSA in wound infections. Our data showed that Manuka honey was effective in the suppression of growth of MRSA strains that are resistant to either one or more than one class of antibiotics. Manuka honey was significantly more effective against strains with the dominant MRSA antibiotic resistance profile (penicillin and oxacillin resistant). However, there were insufficient numbers of isolates for each of the other seven antibiotic susceptibility profiles to definitively conclude if Manuka honey was also more effective for these strains.
Evidence from some studies supports the use of medical-grade honey-based dressings. A prospective observational study was carried out on treatment with Medihoney™ of 121 wounds of various aetiologies during a two-year period in ten hospitals in Germany and Austria [29]. Wound size and perceived pain decreased significantly in response to Medihoney™, wound healing was often rapid and there was less wound slough and/or necrosis [29]. Furthermore, in a pilot study on pin site infections in 21 diabetic patients undergoing Open Reduction with External Fixation (OREF) for correction of Charcot deformity, use of active Leptospermum honey-impregnated dressings significantly reduced the rate of infections [18]. However, other studies suggest caution is needed in the choice of honey-based dressings. For example, results of the randomized controlled HONEYPOT trial do not support the use of topical medical grade honey over topical mupirocin for prevention of exit site infection and peritonitis in adults on Peritoneal Dialysis (PD), although the possibility of benefit in pediatric patients would warrant further specific trials [30].
In Saudi Arabia, where this study was performed, MRSA represents a significant burden both within healthcare facilities and in the community, for example in SSTIs [1, 31-33]. Potentially, the use of medical grade Manuka honey could form a valuable adjunctive treatment along with antibiotics, consistent with experience in other countries. Bacterial biofilms are a particular problem in chronic wound infections, and the efficacy of Medihoney™ against biofilms has been shown in vitro [9, 19]. A recent study using MacSynergy II to study responsiveness of S. aureus biofilms to combinations of Medihoney™ and different antibiotics showed strong synergy between Medihoney™ and rifampicin in reduction of biofilm biomass and embedded cell viability [21]. The extent of the reduction would be likely to have in vivo significance [21]. The study also showed, however, that Medihoney™ at subinhibitory concentrations had antagonistic effects on clindamycin, gentamicin, and oxacillin treatment, indicating the importance of establishing effective concentrations and combinations. Synergism between rifampicin and Medihoney™ against MRSA and clinical isolates of S. aureus has also been shown in checkerboard microdilution assays, time-kill curve experiments and agar diffusion assays, along with a reduction in emergence of rifampicin-resistant S. aureus in vitro, suggesting that use of Medihoney™ as an adjunctive treatment could have benefits in reducing the risk of antibiotic resistance [20]. Other in vitro studies have shown that co-treatment with Manuka honey and oxacillin could synergistically inhibit MRSA in vitro and restore oxacillin sensitivity [34]. Cultivation of bacterial strains including MRSA, P. aeruginosa, E. coli and S. epidermis in the presence of sub-lethal concentrations of Manuka honey and under conditions in which antibiotic-resistance would rapidly develop did not lead to the emergence of honey-resistant bacterial strains [10, 35]. These results suggest an important further advantage to use of medical-grade honey products in the context of the rise of antibiotic resistance [10, 35].
CONCLUSION
In conclusion, locally sourced Germania honey is less effective in vitro than Manuka honey MGO 550 in killing MRSA from patient wound infections. Further studies could be carried out to determine if Germania honey is more effective against other bacterial species. Use of Manuka honey dressings should be considered in MRSA wound dressing in Saudi Arabia.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Johns Hopkins Aramco Healthcare Institutional Review Board.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors wish to acknowledge the use of Johns Hopkins Aramco Healthcare (JHAH) facilities for the data and study for this paper. The opinions expressed in this article are those of the authors and not necessarily of JHAH.

