All published articles of this journal are available on ScienceDirect.

Single-Dose Fosfomycin Trometamol Versus Other Antimicrobial Regimens For Treatment Of Uncomplicated Lower Urinary Tract Infection: A Systematic Review And Meta-Analysis
Abstract
Objectives:
Uncomplicated Lower Urinary Tract Infections (LUTIs) are the most common source of infection affecting women. The increasing prevalence of antimicrobial resistance to commonly prescribed antibiotics has led to the development and use of novel therapies. This current meta-analysis and systematic review evaluate the use of single-dose Fosfomycin-Trometamol (FMT) versus alternative antimicrobial regimens in the management of uncomplicated LUTI.
Methods:
This is a systematic review. We included observational studies and Randomized Controlled Trials (RCTs). Studies that investigated the efficacy of fosfomycin or FMT in managing uncomplicated LUTIs in any age group or gender and compared the treatment to any alternative antibiotic regimen were considered eligible.
Results:
After a comprehensive review of the literature, nineteen studies fulfilled the inclusion criteria. All of the eligible studies (3779 patients) investigated showed no difference between the use of single-dose fosfomycin versus alternative antibiotic regimens for LUTI treatment (OR, 1.003; 95% CI, 0.853-1.181; p = 0.967). The OR remained unchanged but became statistically significant when the random-effects model was used for sensitivity analysis (OR, 1.53; 95% CI, 1.05-2.38; p = 0.04).
Conclusion:
The meta-analysis revealed that there was no significant difference between single-dose FMT and the commonly prescribed antibiotic regimens in LUTI treatment outcomes such as clinical improvement and microbial eradication.
1. INTRODUCTION
Urinary Tract Infections (UTIs) are one of the most frequently encountered bacterial infections in women [1-4], and most commonly present as an acute uncomplicated UTI, relegated to the lower urinary tract. Up to 20-30% of adult women will experience at least one UTIs each year [1]. While there are multiple urinary pathogens responsible for UTIs in women, the most common causative microorganism is Escherichia coli (E. coli), which is the etiological agent in 70–90% of all bacterial LUTIs [2-5]. A range of antibiotics with varied dosing, frequencies and durations have been used to treat uncomplicated UTIs. Although a 7-to-10-day treatment regimen has been the standard practice historically, there is an increasing interest in the use of short-term regimens of 1-3 days. Such regimens are reported to have similar efficacy rates as longer courses with the added benefits of improving patient compliance and reducing adverse events associated with the long term exposure to antimicrobial medications.
The prevalence of antibacterial resistance to antibiotics commonly prescribed for LUTIs varies across countries. These resistance rates are, at least partially, related to the increasingly widespread use of antibiotics [6, 8-11]. The resistance of E. coli and other uropathogens to antimicrobials such as Sulfamethoxazole-Trimethoprim (SXT), ampicillin and the quinolones, have gradually increased in the United Arab Emirates [12-17]. Therefore, novel antibiotics with dosing regimens that are easy to comply with and do not share similar resistance mechanisms to currently available antibiotics are needed. Fosfomycin-trometamol (FMT) is a phosphonic acid derivative that is reported to be as efficacious as other commonly used antimicrobials for the treatment of uncomplicated LUTIs when prescribed as a single three gram dose [18, 19, 21-24].
A single-dose of FMT provides benefits over antibiotics with multiple dose regimens due to its minimal side-effects and excellent safety profile when prescribed to children and pregnant women [23-29].
The goal of this systematic review is to evaluate the clinical and microbial efficacy of single-dose FMT versus traditional antimicrobial regimens in a diverse group of patients presenting with uncomplicated LUTIs.
2. MATERIALS AND METHODS
2.1. Search Strategy
We completed a comprehensive systematic review via MEDLINE and the Cochrane Library, with no restrictions based on language or year of publication. The search string used was: (fosfomycin OR fosfomycin trometamol) and urine. The final search occurred in June 2018. Additional articles relevant to the study were manually obtained by reviewing the reference lists of eligible bibliographies and the reference section of selected manuscripts was investigated to make sure that all publications relevant to the topic were utilized.
2.2. Study Selection
Studies that investigated the efficacy of fosfomycin or FMT in managing uncomplicated LUTIs in any age group or gender and compared the treatment to any alternative antibiotic regimen were considered eligible. Studies were eligible for inclusion into the meta-analysis if they evaluated single-dose fosfomycin or FMT as monotherapy in comparison to other antimicrobials. Studies that did not report clinical or bacterial culture outcomes were excluded from the analysis. In addition, studies without an English translation or publically available full text were also excluded.
2.3. Data Extraction and Quality Assessment
Two reviewers (M.A and K.I.) independently evaluated the data using a predetermined screening form. If a disagreement in study eligibility arose, the reviewers re-assessed the data until consensus was reached. We extracted the following data from each study: the primary author’s last name, year of publication, country in which the study took place, study type (retrospective/prospective, cohort/case-control/randomised), matching criteria (for case-control studies), authors’ definition of uncomplicated LUTI, fosfomycin dose, type and dose of alternate antimicrobials, therapy length, etiological microorganism(s), comorbid patient conditions and defining outcomes (clinical and microbiological).
Each study was independently assessed by the investigators to determine methodological quality for cohort or case control studies and randomized studies, using the Newcastle-Ottawa Quality Assessment Scale [12] and the Cochrane risk-of-bias tool assessment [13], respectively.
2.4. Outcome Measures
The main outcome measurement was the clinical success rate, defined as clinical cure or improvement (complete and partial resolution, respectively) of the signs and symptoms of LUTI at the termination of the prescribed antimicrobial regimen.
The secondary outcome measures were infection-related mortality, overall mortality, nephrotoxicity and eradication of the microbial organisms, which were defined as undetectable growth of the etiological agent at the end of the prescribed antimicrobial regimen, irrespective of the clinical outcome.
2.5. Data Synthesis and Analysis
The pooled effect estimates and their 95% Confidence Interval (CI) were determined only when two or more studies with sufficient data were available for each outcome of interest. The overall effect estimate for all dichotomous data with 95% CI was calculated as the Odds Ratio (OR). The presence of statistical heterogeneity among the studies and the magnitude of heterogeneity were addressed by utilizing Q and I2 statistics, respectively. A p value less than 0.10 or an I2 value greater than 50% was determined to signify substantial heterogeneity. In the cases that substantial heterogeneity was observed and not observed, pooled OR was calculated by the random-effects and fixed-effects models, respectively. We used Comprehensive Meta-Analysis version 3.3.070 for all calculations.
The exclusion criteria were conducted based on sensitivity analysis and were determined by recalculating pooled OR estimates for each study subgroups based on the relevant clinical characteristics. This analysis indicates if the overall results were affected by changing the selection criteria for meta-analysis. As the eligible studies were clinically heterogeneous, we performed sensitivity analysis on all outcomes by the utilizing random-effects model regardless of the estimate of statistical heterogeneity.
3. RESULTS
3.1. Searching Results
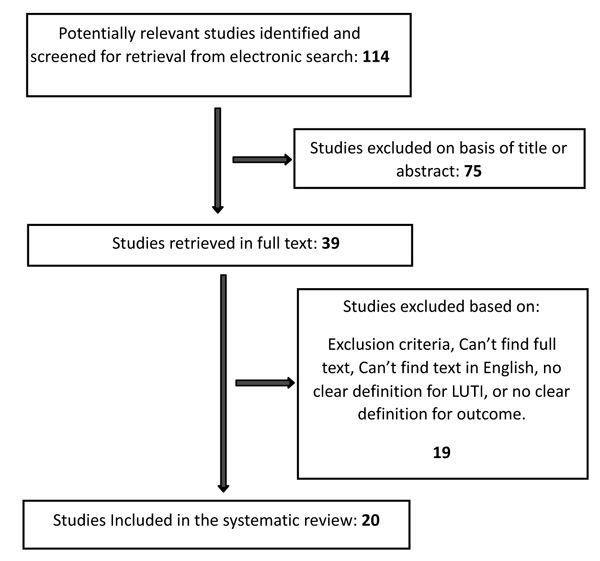
The systemic review identified 114 relevant records, of which 38 full-text manuscripts were determined to be potentially eligible. Only 19 of these articles met the full inclusion criteria for our study. Fig. (1).
3.2. Meta-Analysis and Quality Assessment of the Eligible Studies
Among the 19 studies included in our analysis (see Table 1), 18 compared the use of single-dose fosfomycin versus alternate antibiotics while one study compared two doses of fosfomycin with alternate antibiotics. Seventeen of the studies used the same definition of uncomplicated LUTI. A single study used acute UTI as the defining illness.
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) evidence profile was used to assess the quality of evidence for each outcome in the meta-analysis. The GRADE results did not reveal any limitations in the study design or inconsistency in the majority of outcomes of the studies evaluated. There was no observed indirectness or imprecision in the reporting of results. Based on these assessments, we considered the quality of evidence for each outcome to be moderate.
3.3. Systematic Review of the Eligible Studies
Sixteen of the eligible studies used a single-blinded design, while the remainder used a randomised double-blinded design. Eight studies reported on both the clinical and microbiological outcomes, while 11 studies only reported on microbiological outcomes. Of the 19 eligible studies, four compared fosfomycin to norfloxacin, three compared it to trimethoprim, two each compared it to ciprofloxacin, nitrofurantoin, amoxicillin-clavulanate and pipemidic acid and one each compared it to cephalexin, pefloxacin, netilmicin and cephalexin. The quality of evidence was considered moderate based on the GRADE approach.
3.4. Clinical Outcome: Clinical Response with Single-dose Fosfomycin Versus Alternate Antibiotic Regimens
Eight studies, consisting of 2886 patients, evaluated the clinical response of patients with LUTI who received single-dose fosfomycin treatment in comparison with patients who received alternate antimicrobial regimens. Consistency in the definition of clinical response was observed among all eligible studies.
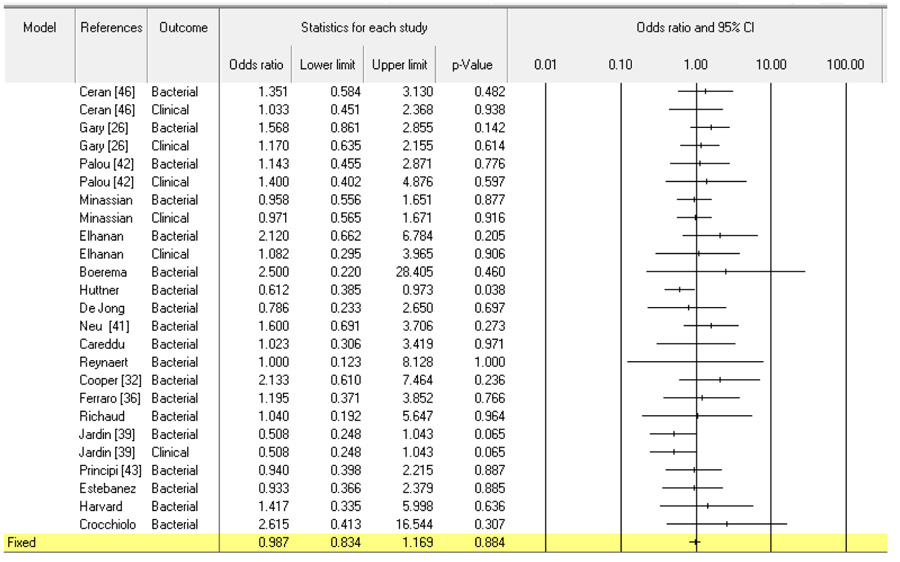
A non-statistically significant improvement in clinical outcomes was found when alternative antibiotic regimens were compared to single-dose fosfomycin (OR, 0.957; 95% CI, 0.717-1.276; p = 0.764). This result indicates that there was no difference between the two groups (Fig. 2). The quality of evidence for this outcome was considered moderate based on the GRADE approach. The OR remained unchanged but statistically significant when the random-effects model was used for sensitivity analysis (OR, 1.53; 95% CI, 1.05–2.38; p = 0.04).
3.5. Microbiological Outcome: Microbiological Eradication with Single-dose Fosfomycin Versus Alternate Antibiotic Regimens
All of the eligible studies (3779 patients) evaluated data on the microbiological eradication of single-dose fosfomycin compared to alternative antibiotic regimens. There was consistency across the included studies in the definition of clinical success.
A non-statistically significant improvement in clinical response was found when single-dose fosfomycin was compared to alternate antibiotic regimens (OR, 1.026; 95% CI, 1.250-0.798; p = 0.798). This result indicates that there was no difference between the two groups (Fig. 2). According to the GRADE approach, the quality of evidence for this outcome was moderate. The OR remained unchanged but became statistically significant when the random-effects model was used to determine sensitivity analysis (OR, 1.53; 95% CI, 1.05-2.38; p = 0.04).
| Publication year | Reference number | Location | Study type | Setting | Infection type | Antibiotic Compared with | Duration(FSM, ABX) | Number of patients | Clinical Outcome | Microbiological Oucome | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FSM | ABX | FSM | ABX | |||||||||
| 2010 | 31 | Turkey | randomized, single-blind design | Hospital | Uncomplicated UTIs | Ciprofloxacin | 1, 5 | 142 | 62/77 | 52/65 | 64/77 | 51/65 |
| 1999 | 26 | USA | randomized double blinded trial | Multi center | Uncomplicated UTIs | Nitrofurantoin | 1, 7 | 749 | 207/229 | 193/217 | 146/168 | 127/157 |
| 2013 | 42 | Spain | randomized, single-blind design | Multi center | Uncomplicated UTIs | Ciprofloxacin | 2, 3 | 118 | 32/37 | 32/39 | 23/37 | 23/39 |
| 1998 | 40 | UK | randomized, single-blind design | Hospital | Uncomplicated UTIs | TMP | 1, 5 | 547 | 139/195 | 69/96 | 147/204 | 70/96 |
| 1994 | 45 | Jerusalem | randomized, single-blind design | Hospital | Uncomplicated UTIs | Cephalexin | 1, 5 | 130 | 53/58 | 49/54 | 53/58 | 45/54 |
| 1990 | 27 | Netherlands | randomized, double-blind design | Hospital | Uncomplicated UTIs | Norfloxacin | 1, 7 | 158 | 55/60 | 48/50 | 60/61 | 48/50 |
| 2018 | 38 | Europe | randomized, single-blind design | Multi center | Uncomplicated UTIs | Nitrofurantoin | 1, 5 | 513 | 139/241 | 171/244 | 103/163 | 129/175 |
| 1991 | 34 | France | randomized, single-blind design | Hospital | Uncomplicated UTIs | Norfloxacin | 1, 5 | 63 | NA | NA | 22/30 | 21/27 |
| 1990 | 41 | USA | randomized, single-blind design | Hospital | Uncomplicated UTIs | Amoxycillin | 1, 1 | 158 | NA | NA | 52/65 | 40/56 |
| 1987 | 39 | Italy | randomized, single-blind design | Hospital | Uncomplicated UTIs | Pipemidic acid | 1, 7 | 51 | NA | NA | 17/24 | 19/27 |
| 1990 | 44 | Belguim | randomized, single-blind design | Hospital | Uncomplicated UTIs | Norfloxacin | 1, 3 | 32 | NA | NA | 14/16 | 14/16 |
| 1990 | 32 | UK | randomized, single-blind design | Hospital | Acute UTI | Amoxicillin/clavulanic acid | 1. 5 | 141 | NA | NA | 28/33 | 21/29 |
| 1990 | 36 | Italy | randomized, single-blind design | Hospital | Uncomplicated UTIs | Norfloxacin | 1, 7 | 60 | NA | NA | 23/30 | 22/30 |
| 1995 | 30 | France | randomized, single-blind design | Hospital | Uncomplicated UTIs | Pefloxacin | 1, 1 | 57 | NA | NA | 26/29 | 25/28 |
| 1990 | 39 | France | randomized, single-blind design | Multi center | Uncomplicated UTIs | Pipemidic acid | 1, 5 | 386 | 122/146 | 130/143 | 122/146 | 130/143 |
| 1990 | 43 | Italy | randomized, single-blind design | Hospital | Uncomplicated UTIs | Netilmicin | 1, 1 | 135 | NA | NA | 57/71 | 52/64 |
| 2009 | 35 | Spain | randomized, single-blind design | Hospital | Uncomplicated UTIs | Amoxicillin-clavulanate | 1, 7 | 109 | NA | NA | 42/53 | 45/56 |
| 2010 | 31 | Turkey | randomized, single-blind design | Hospital | Uncomplicated UTIs | Ciprofloxacin | 1, 5 | 142 | 64/77 | 53/65 | 64/77 | 51/65 |
| 1990 | 37 | UK | randomized, double-blind design | Hospital | Uncomplicated UTIs | Trimethoprim | 1, 1 | 51 | NA | NA | 17/22 | 12/017 |
| 1990 | 33 | Italy | randomized, single-blind design | Multi center | Uncomplicated UTIs | Cotrimoxazole | 1, 3 | 36 | NA | NA | 17/19 | 13/17 |
3.6. Overall Outcome: Single-dose Fosfomycin Versus Alternate Antibiotic Regimens for LUTI Treatment
All of the eligible studies (3779 patients) investigated showed no difference between the use of single-dose fosfomycin versus alternative antibiotic regimens for LUTI treatment (OR, 1.003; 95% CI, 0.853-1.181; p = 0.967). The OR remained unchanged but became statistically significant when the random-effects model was used for sensitivity analysis (OR, 1.53; 95% CI, 1.05-2.38; p = 0.04).
4. DISCUSSION
The optimal antimicrobial treatment duration for uncomplicated LUTI depends on a host of factors. Short (1–3 days) courses of therapy appear to be the most effective in young, non-pregnant women who present with symptoms lasting less than 7 days and who do not have a recent history of failed treatment. Interestingly, short courses of therapy are associated with worse outcomes in uncomplicated LUTIs caused by Staphylococcus saprophyticus, the second most common bacteria found in young women presenting with UTIs.
Single-dose regimens are not the standard of care as many antimicrobials, especially the beta-lactam group, have reduced efficacy when prescribed as a single dose, even in the case of supratherapeutic doses [14]. Furthermore, UTI symptoms often persist beyond a single day of treatment, which may produce anxiety in patients who fear that their antimicrobial treatment course is inadequate.
FMT is a unique antibiotic in that it is an effective single-dose therapy in women age 18 years and older with acute uncomplicated LUTI [16]. Results of small clinical trials indicate that clinical cure and microbial eradication with FMT is equivalent to comparable antibiotic agents, such as norfloxacin and STX when administered for periods of 1, 3, 5 or 7 days.
The present study is a systematic review and meta-analysis that primarily examines the role of single-dose fosfomycin in the management of LUTIs. Our findings indicate that there is no significant difference between single-dose fosfomycin and alternate antibiotic regimens for the treatment of LUTI related outcomes, including clinical cure, improvement and microbiological eradication.
CONCLUSION
This meta-analysis suggests that single-dose fosfomycin is an effective treatment modality for uncomplicated LUTI.
CONSENT FOR PUBLICATION
Not applicable.
STANDARD FOR REPORTING
PRISMA guidelines and methodology were followed.
AVAILABILITY OF DATA AND MATERIALS
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
We would like to extend our thanks to the Medical College, University of Sharjah for UAE supporting this study.

