All published articles of this journal are available on ScienceDirect.

Molecular Study of Enterotoxins Genes of Staphylococcus aureus Isolated from Patients in Intensive Care Units
Abstract
Introduction:
Staphylococcus aureus is responsible for healthcare-associated sepsis. Various virulence genes may be responsible for the severity of the outcome of this infection.
Aims & objectives:
Therefore, the aim of the present study was to investigate the prevalence of enterotoxin genes in S .aureus associated with HCA sepsis affecting adult's patients in Intensive Care Units (ICU).
Materials & Methods:
The study is a cross-sectional observational study included 432 patients admitted to intensive care units with Healthcare-Associated Infections (HCAIs). The patients were subjected to blood culture and identification of the isolated bacteria according to the standard microbiological method. Isolates identified as S. aureus were subjected to molecular studies for the detection of meca gene and enterotoxins genes by multiplex Polymerase Chain Reaction (PCR).
Results & Discussion:
Blood culture was positive in 170 of the patients (39.3%). 47 of the blood culture yield S. aureu. Regarding studies of virulence genes in isolated S. aureus, the most frequent genes were seg (61.7%), mecA (46.8%) and sea (42.6%). The less frequent genes were tst and eta 6.4% for each. Analysis of demographic, clinical and virulence genes of isolated S. aureus to HAIs outcome reveals that the virulence genes namely mec, sei and tst of S. aureus were the only significant factors associated with death The distribution of enterotoxigenic genes among MRSA and MSSA shows a significant association between seg and sei genes in MRSA isolates.
Conclusion:
The present study highlights the prevalence of enterotoxin genes in isolated S.aureus from patients with hospital-acquired infections in intensive care units in a tertiary hospital. There was high prevalence as about two-thirds of the isolates harbor seg and sea genes in addition to methicillin resistance gene mecA. The fatal outcome of sepsis in those patients was associated with the presence of enterotoxin genes sei and tst. There is a need for screening patients admitted to intensive care units for S. aureus harboring these genes for proper management and application of isolation and contact guidelines of infection control
1. INTRODUCTION
Staphylococcus aureus (S.aureus) is a widely distributed pathogen, while it represents important colonizing bacteria in the anterior nares of about one-third healthy population [1]. S. aureus represents a major cause of infections in community-acquired and in Healthcare-Associated Infections (HCAIs) such as sepsis, endocarditis and soft tissue infections [2, 3]. The consequences of the infections by S. aureus have increased by the development of antibiotics resistance especially to methicillin with widespread Methicillin-Resistant S. Aureus (MRSA) among HCAI [4].
Sepsis caused by MRSA is defined as the second common cause of death in Europe and representing around 25% of death in the United States of America [4].
The pathogenicity of S. aureus is associated by many factors such as multiple antibiotics resistance pattern especially of MRSA strains and the presence of several virulence factors and toxins production associated with some strains. The risk factors for acquiring HCAI associated with virulent S.aureus strains include prolonged hospitalization, prior antibiotics use, presence of prosthetic or central line, presence of immunocompromizing conditions such as diabetes mellitus and malignancy [5].
Staphylococcus aureus has several virulence factors such as the microbial surface components that facilitate the adhesion of the bacteria to the prosthetic surfaces in addition to the secreted toxins and adhesion factors like hemolysins, leukocidins, enterotoxins, and exfoliative toxins that aid in invasion and spread of infection [6].
The toxicity of the produced toxins from S. aureus is associated with superantigens properties that lead to massive immune reactions such as that associated with enterotoxins production. The superantigens act by the release of massive proinflammatory cytokines that lead to massive inflammatory reactions. Superantigens act by direct strong activation of T lymphocytes without prior antigen presentation; it acts by binding to a specific variable region of the T cell antigen receptor-β-chain [7]. This leadsto a massive release of proinflammatorycytokines such as TNF-α, IL-6, and IFN-γ [8, 9]. This systemic inflammatory reaction can contribute to the severity of S. aureus sepsis [10].
Therefore, the aim of the present study was to investigate the prevalence of enterotoxin genes in S. aureus associated with HCA sepsis affecting adult's patients in Intensive Care Units (ICU) from Mansoura University Hospital, Egypt from May 2017 till April 2018.
2. MATERIALS AND METHODS
The study is a cross-sectional observational study conducted on Mansoura University Hospital, Egypt from May 2017 till April 2018. Patients were admitted to intensive care units in the hospital during this period. The study was approved by Mansoura Faculty of Medicine ethical committee and approval consents were obtained from the patients.
The patients were subjected to full clinical history registration by smartphone as a part of the national surveillance system of the infection control committee of Universities hospitals in cooperation with Center of Disease Control (CDC)-USA for hospital-acquired infections-phase 3. The registered data included demographic data, presence of comorbidity, cause of admission, presence of organ failure associated with sepsis, the signs associated with sepsis and the outcome either by discharge or death. The sepsis was identified as primary sepsis with no signs of other focus of infections; device associated bloodstream infections associated with the use of the devices such as a central venous catheter and secondary sepsis if there was the primary focus of infection.
2.1. Microbiological Culture
Ten Milliliter blood samples were collected from each patient completely under sterile conditions. Five milliliters of the blood was inoculated to aerobic blood culture and the other five was inoculated to the anaerobic blood culture bottles (BD BACTEC™ FX blood culture system). Positive blood culture bottles were subjected to subculture on blood agar at 37ºC for 24-48 hours. Colonies were subjected to identification by gram stain, coagulase and catalase tests for identification of S. aureus.
Antibiotics susceptibility tests were performed by disc diffusion method on Muller –Hinton agar according to the Clinical and Laboratory Standards Institute (CLSI) 2013 [11]. The used discs were imipenem (10μg/disk), amikacin (30µg), amoxicillin/clavulinic acid (30µg), ampicillin(10µg),ciprofloxacin (10μg), cefotaxime (30µg), ceftazidime (10µg), cefoxitin (10µg), trimethoprim/sulfamethaxone (25µg) erythromycin (15µg) (Oxoid-Thermo Fisher Scientific- Thermo Fisher Scientific 168 Third Avenue,Waltham, MA USA 02451). MRSA was defined as S. aureus resistant to cefoxitin.
2.2. Molecular Studies of Isolated S. aureus
2.2.1. DNA Extraction
The colonies that were identified to be S. aureus were subcultured on blood agar plates at 37ºC for overnight and the colonies were obtained and DNA was extracted by the boiling method as described previously [12].
DNA was kept frozen at -20ºC till PCR.
2.2.2. Duplex PCR for Identification of MRSA
Identification of MRSA was performed by rapid duplex PCR described previously by Jonas et al., 2002 [13]. The principle of PCR is the use of four primers for mecA and femB in PCR. Positive isolates for both genes indicated MRSA. The sequences of the used primers were listed in Table 1.
| Genes | Sequences | bp |
|---|---|---|
| MRSAmecAfemB | 5′-GTA GAA ATG ACT GAA CGT CCG ATA A-/35′-CCA ATT CCA CAT TGT TTC GGT CTA A-/35′-TTA CAG AGT TAA CTG TTA CC-/35′-ATA CAA ATC CAG CAC GCT CT-/3 | 310-bp651-bp |
| Enteotoxin-Mixture ASeaSebSecSedSeefemAEnterotoxin-mixture BEtaetbtst | 5′-GGTTATCAATGTGCGGGTGG-/35′-CGGCACTTTTTTCTCTTCGG-/35′-GGTTATCAATGTGCGGGTGG-/35′-CGGCACTTTTTTCTCTTCGG-/35′-AGATGAAGTAGTTGATGTGTATGG-/35′-CACACTTTTAGAATCAACCG-/35′-CCAATAATAGGAGAAAATAAAAG-/35′-ATTGGTATTTTTTTTCGTTC-/35′-AGGTTTTTTCACAGGTCATCC-/35′-CTTTTTTTTCTTCGGTCAATC-/35′-AAAAAAGCACATAACAAGCG-/35′-GATAAAGAAGAAACCAGCAG-/35′-GCAGGTGTTGATTTAGCATT-/35′-AGATGTCCCTATTTTTGCTG-/35′-ACAAGCAAAAGAATACAGCG-/35′-GTTTTTGGCTGCTTCTCTTG-/35′-ACCCCTGTTCCCTTATCATC-/35′-TTTTCAGTATTTGTAACGCC-/3 | 10216445127820913293226326 |
The amplification process included denaturation at 94°C for 4 minutes (min), followed by 30 cycles of 45 seconds at 94°C, 45 seconds at 50°C, and 60 seconds at 72°C, with a final extension step at 72°C for 2 min. Ten microliter aliquots were loaded onto agarose gel electrophoresis 90 V for 90 minutes and stained with 10 μg of ethidium bromide/ml after electrophoresis.
2.2.3. Multiplex PCR for Enterotoxins Detection
Multiplex PCR was used by preparing a mixture A set with the primers mentioned in Table 1 and primers mixture B (Qiagen). The first reaction of PCR contained 10ng of template DNA with 20picomol (each) of sea, seb, sec, see, and femA primers in amplification mixture of 50 μl of the ready to use Qiagen amplification mixture. The second round of PCR, the primers used, were those for B mixture at a concentration of 20 pmol each for etb, tst, and femA and 50 pmol for eta. The following amplification steps were carried out in the first round and in the second round of PCR; denaturation at 94°C for 5 min was followed by 35 cycles of amplification (denaturation at 94°C for 2 min, annealing at 57°C for 2 min, and extension at 72°C for 1 min), ending with a final extension at 72°C for 7 min [14].
2.2.4. Quality Control for PCR
The strains used as positive control for PCR reactions were S. aureus ATCC 13565 (SEA), S. aureus ATCC 14458 (SEB), S. aureus ATCC 19095 (SEC), S. aureus90-S-1025 (SED), S. aureusATCC 27664 (SEE), S. aureus 88-S-8902 (ETA), S. aureus 88-S-8620 (ETB), S. aureus 92-S-1344 (TSST-1), and S. aureus 95-S-739 (mecA). Sterile distilled water was used as negative control.
2.2.5. Statistical Analysis
Data were collected, revised, coded and entered to the statistical package for social science (SPSS) version 20. The quantitative data were presented as mean, standard deviations and ranges. The comparison between the studied groups was done by using Chi-Square and P was considered significant when < 0.05.
3. RESULTS
The study included 432 patients admitted to intensive care units and suspected to have HCAIs. Blood culture was positive in 170 of the patients (39.3%). 47 of the blood culture yield S .aureus, data not shown.
The study of demographic and clinical data associated with HAIs due to S. aureus was summarized in Table 2. The patients were mainly female patients (53.2%) with mean age 52.6± 11.3 years. The main diagnostic sign was fever (80.9%) and hypotension (46.8%). The infection was associated with the presence of central venous catheter in 14.9% of the patients, ventilator in 4.3% and urinary catheter in 2.1%. The type of the HAIs was primary sepsis in 48.9% of the patients followed by secondary sepsis due to pneumonia in 34% of the patients and urinary tract infections in 17% of the patients. The outcome of the patients discharged in 61.7% and death in 38.3% of the patients, Table 2.
| Age (mean SD) Years | 52.6± 11.3 |
|---|---|
| Gender Male – No.-% Female– No.-% |
22 46.7% 25 53.2% |
| Diagnosis at admission Malignancy– No.-% COLD\– No.-% Infection– No.-% Diabeteiusmelliteus– No.-% |
11 23.4% 10 21.3% 18 38.3% 8 17.00% |
| Fever – No.-% | 38 80.9% |
| Hypotension– No.-% | 22 46.8% |
| Renal insufficiency– No.-% | 6 12.6% |
| Association with device No– No.-% Central– No.-% Urinary catheter– No.-% Ventilator– No.-% |
37 78.7% 7 14.9% 1 2.1% 2 4.3% |
| Type of HAIs Sepsis– No.-% Pneumonia– No.-% Urinary tract infections– No.-% |
23 48.9% 16 34% 8 17% |
| Outcome Discharge– No.-% Death– No.-% |
29 61.7% 18 38.3% |
| Total | 47 |
Regarding studies of virulence genes in isolated S. aureus, the most frequent genes were seg (61.7%), mecA (46.8%) and sea (42.6%). The less frequent genes were tst and eta (6.4%) for each, Table 3.
| Gene | No. % |
|---|---|
| mecA | 22 46.8 |
| sei | 15 31.9% |
| sea | 20 42.6 |
| seg | 29 61.7% |
| tst | 3 6.4% |
| eta | 3 6.4% |
Analysis of demographic, clinical and virulence genes of isolated S. aureus to HAIs outcome reveals that the virulence genes namely mec, sei and tst of S.aureus were the only significant factors associated with death (P=0.0001, P=0.0001, P=0.05 respectively), Table 4.
| Characteristics | Death (n=18) |
Survivors (n=29) |
P |
|---|---|---|---|
| Male-No.-% Female-No.-% |
8 44.4% 10 55.6% |
14 48.3% 15 51.7% |
P=0.8 |
| Age (mean± SD)years | 49.2± 17.4 | 54.7± 17.3 | P=0.3 |
| Diagnosis at admission Malignancy No.-% COLD No.-% Infection No.-% Diabeteiusmelliteus No.-% |
5 27.8% 2 11.1% 9 50% 2 11.1% |
6 20.7% 8 27.6% 9 31.0% 6 20.7% |
P=0.3 |
| Type of HAIs Sepsis No.-% Pneumonia No.-% Urinary tract infections No.-% |
8 44.4% 7 38.9% 3 16.7% |
15 51.7% 9 31.0% 5 17.2% |
P=0.9 |
| Association with device No No.-% Central No.-% Urinary catheter No.-% Ventilator No.-% |
13 72.2% 3 16.7% 0 0.0% 2 11.1% |
24 82.8% 4 13.8% 1 3.4% 0 0% |
P=0.3 |
| Fever No.-% | 15 83.3% | 23 79.3% | P=0.5 |
| Hypotension No.-% | 10 55.6% | 12 41.4% | P=0.3 |
| Renal insufficiency No.-% | 5 27.8 | 1 3.6% | P=0.2 |
| MesNo.-% | 15 83.3% | 7 24.1% | P=0.0001 |
| sea | 10 55.6% | 10 34.5% | P=0.2 |
| seg | 16 88.9% | 2 6.9% | P=0.0001 |
| Sei | 14 77.8% | 1 3.4% | P=0.0001 |
| eta | 1 5.6% | 0 0% | P=0.1 |
| tst | 3 16.7% | 0 0% | P=0.05 |
The distribution of enterotoxigenic genes among MRSA and MSSA shows a significant association between seg and sei genes in MRSA isolates, Table 5.
| - | MRSA (n=22) |
MSSA (n=25) |
P |
|---|---|---|---|
| sea | 10 45.5% | 10 40% | P=0.3 |
| seg | 14 63.6% | 4 16% | P=0.001 |
| sei | 12 54.5% | 3 12% | P=0.002 |
| Eta | 2 9.1% | 1 4% | P=0.3 |
| tst | 3 13.6% | 0 0% | P=0.1 |
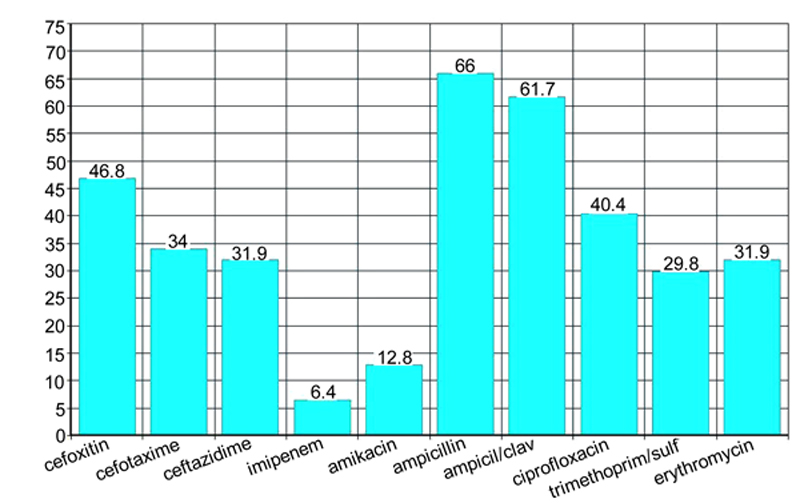
Isolated S. aureus from blood culture had high resistance to betalactam antibiotics, ampicillin, amoxicillin/clavulinic acid (66%, 61.7% respectively). The lowest resistance was for imipenem followed amikacin (6.4%, 12.8% respectively), (Fig. 1).
4. DISCUSSION
The site of infections in ICU depends upon different factors such as the type of ICUs, the type of the patients served by the hospital and the method of surveillance depending method for identification of HAIs [15]. In the present study, the surveillance method was performed by active detection of the clinical signs of infections for patients admitted to ICUs associated with laboratory diagnosis. The rate of positive blood culture for those patients(39.3%) was higher than the previously reported rate [16]. However, the results were consistent with the reports determining that sepsis as one of the common hospital-acquired infections with pneumonia and urinary tract infections [16, 17].
The practice of patients care has many advances in the last decades among which are the use of invasive devices. The invasive devices such as central venous line and urinary catheters are associated with the introduction of virulent pathogens from the surrounding environment to patients with reduced immune states due to their diseases and associated comorbidity [18]. In the present study, the sepsis was associated with a central venous catheter in 14.9%, ventilator in 4.3% and urinary catheter in 2.1%. These rates were higher than that reported previously by Sato et al., 2016 [19] (3.4%) and lower than that reported by Braga et al. [17], (87.%). The differences may be attributed to the difference in the site of infections and the types of ICUs. Moreover, there are differences in the compliance of healthcare workers to guidelines for infection control.
In the present study, S. aureus was isolated from 27.6% of positive blood culture. S. aureus is considered one of the most important pathogens, responsible for nosocomial infections. The prevalence rate of S. aureus was similar to a previous report [20].
The prevalence of MRSA strains among isolated S. aureus was around half of the isolates. This finding is online with the previous report from USA with rates up to 55% of isolated S.aureus defined as MRSA [21]. MRSA is associated with high mortality rates among patients admitted to ICUs, higher costs and prolonged hospital stay [21].
Regarding studies of virulence genes in isolated S. aureus, the most frequent genes were seg (61.7%), and sea (42.6%). The less frequent genes were tst and eta (6.4% for each). Different reports defined sea and seg genes as the most frequent enterotoxins genes associated with hospital-acquired sepsis [22]. Other report found tst and txt as the common enterotoxin genes in S. aureus isolates [23]. The distribution of enterotoxin genes differs according to geographic regions and types of studied patients.
The distinguished findings of the present study were the statistically significant association of the virulent genes mec, sei and tst of S. aureus with death.
Enterotoxins in S. aureus are associated with septic shock as they are known to be a strong inducer of the adaptive immune system as they act as a superantigen [17]. There are strong evidence for this action in animals models, however, human studies are scarce [24, 25]. The prevalence of specific enterotoxines genes of S. aureus among patients in different geographic location is not well known [25].
Isolated S. aureus from blood culture had high resistance to beta-lactam antibiotics, ampicillin, amoxicillin/clavulinic acid (66%, 61.7% respectively). The lowest resistance was for imipenem followed amikacin (6.4%, 12.8% respectively).
Staphylococcus aureus and especially MRSA strains have shown an increase resistance towards currently available beta-lactam antimicrobial agents such as penicillin and cephalosporins [26]. The microbiological study of antibiotics susceptibility pattern is an important issue to control infection with ICU by use of empiric therapy based upon locally prepared antibiotics policy. Other measures to control the spread of S .aureus is good hand hygiene practice and proper isolation precautions for patients infected with MRSA with active surveillance of the patients admitted to ICU to enhance contact precautions [27, 28].
CONCLUSION
The present study highlights the prevalence of enterotoxin genes in isolated S. aureus from patients with hospital-acquired infections in intensive care units in a tertiary hospital. There was high prevalence as about two-thirds of the isolates harbor seg and sea genes in addition to methicillin resistance gene mecA. The fatal outcome of sepsis in those patients was associated with the presence of enterotoxin genes sei and tst. There is a need for screening patients admitted to intensive care units for S. aureus harboring these genes for proper management and application of isolation and contact guidelines of infection control.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by Mansoura Faculty of Medicine committee.
HUMAN AND ANIMAL RIGHTS
No animals/humans were used for studies that are the basis of this research.
CONSENT FOR PUBLICATION
Informed consent were obtained.
CONFLICT OF INTEREST
The author declares no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

